

Intraductal tubulopapillary neoplasm (ITPN) of the pancreas associated with an invasive component: a case report with review of the literature
- PMID: 29145864
- PMCID: PMC5689171
- DOI: 10.1186/s12957-017-1267-4
Intraductal tubulopapillary neoplasm (ITPN) of the pancreas associated with an invasive component: a case report with review of the literature
Abstract
Background: Intraductal tubulopapillary neoplasm (ITPN) depicts a distinct entity in the subgroup of premalignant epithelial tumors of the pancreas. Although the histomorphological and immunophenotypical characterization of ITPN has been described by several authors in terms of report of case series in the past, the rarity of that tumor subtype and similarity to other entities still makes identification of ITPN a challenge for radiologists and pathologists. To date, little is known about tubulopapillary carcinoma that can evolve from ITPN.
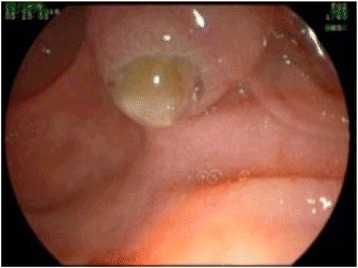
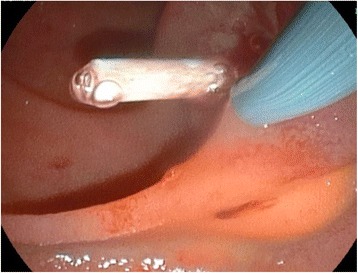
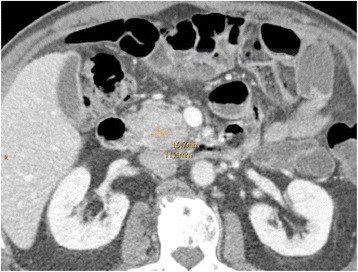
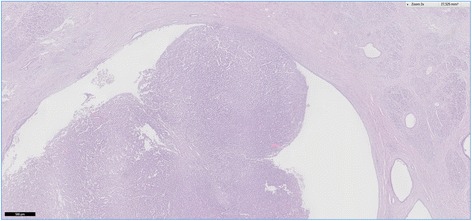
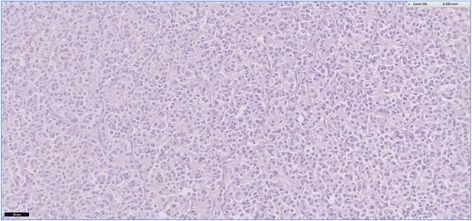
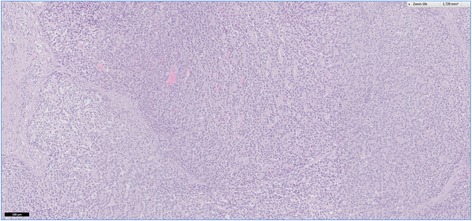
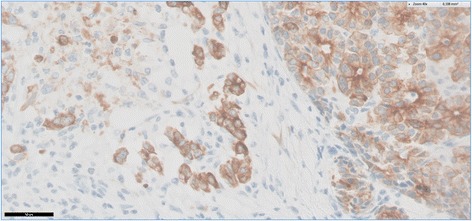
Case presentation: In the present work, we analyze one case of ITPN associated with an invasive component and discuss the results involving the current literature. Collected patient data included medical history, clinical symptoms, laboratory tests, radiological imaging, reports of interventions and operation, and histopathological and immunohistochemical examinations. The patient initially presented with acute pancreatitis. A solid tumor obstructing the main pancreatic duct and sticking out of the papilla of Vater was detected and caught via endoscopic intervention. Histopathological examination of the specimen revealed mainly tubular growth pattern with back to back tubular glands. Immunohistochemically, the tumor was strongly positive for keratin 7 (CK7) and pankeratin AE1/AE3, and alpha 1 antichymotrypsin; negative for synaptophysin and chromogranin A, CDx2, CK20, S100, carcinoembryonic antigen (CEA), MUC 2, MUC5AC, and somatostatin; and in part positive for CA19-9. Extended pancreatoduodenectomy was performed, the final diagnosis was tubulopapillary carcinoma grown in an ITPN.
Conclusion: The identification of an ITPN of the pancreas can be a challenging task. Endoscopic retrograde cholangiopancreaticography is an excellent tool to directly see and indirectly visualize the intraductal solid tumor and to take a biopsy for histopathological evaluation at the same time. Together with a thorough immunohistochemical workup, differential diagnoses can be ruled out quickly. To date, reports of ITPN are rare and little is known about the potential for malignant transformation and the prognosis of tubulopapillary carcinoma grown from an ITPN. Radical surgical resection following oncologic criteria is recommended; however, more data will be needed to assess an adequate treatment and follow-up standard.
Keywords: Carcinoma; Intraductal; Neoplasia; Pancreas; Pancreaticoduodenectomy.
Conflict of interest statement
Author’s information
The first author, Stefanie Kuscher, is a surgical resident with special interest in pancreas pathologies, respectively pancreas surgery, and a research focus on those topics.
Ethics approval and consent to participate
Not applicable
Consent for publication
The patient was informed about the intention to publish a report of his medical case including anonymized images, without publication of personal data such as name, date of birth, or address. All questions could be answered in the conversation and the patient personally signed the consent form.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures




Similar articles
-
A case of intraductal tubulopapillary neoplasm of the pancreas in a branch duct: a rare case report and literature review.BMC Gastroenterol. 2021 Apr 13;21(1):162. doi: 10.1186/s12876-021-01744-2. BMC Gastroenterol. 2021. PMID: 33849435 Free PMC article. Review.
-
A case of MUC5AC-positive intraductal neoplasm of the pancreas classified as an intraductal tubulopapillary neoplasm?Pathol Res Pract. 2015 Dec;211(12):1034-9. doi: 10.1016/j.prp.2015.10.009. Epub 2015 Oct 30. Pathol Res Pract. 2015. PMID: 26586167
-
An extremely rare case who underwent total remnant pancreatectomy due to recurrent pancreatic metastasis of intraductal tubulopapillary neoplasm.Clin J Gastroenterol. 2019 Apr;12(2):153-159. doi: 10.1007/s12328-018-0913-x. Epub 2018 Oct 4. Clin J Gastroenterol. 2019. PMID: 30284703
-
Intraductal tubular papillary neoplasm (ITPN), a novel entity of pancreatic epithelial neoplasms and precursor of cancer: A case report and review of the literature.Int J Surg Case Rep. 2019;55:187-191. doi: 10.1016/j.ijscr.2019.01.036. Epub 2019 Feb 5. Int J Surg Case Rep. 2019. PMID: 30753991 Free PMC article.
-
Intraductal Tubulopapillary Neoplasm of the Pancreas: An Update From a Pathologist's Perspective.Arch Pathol Lab Med. 2016 Oct;140(10):1068-73. doi: 10.5858/arpa.2016-0207-RA. Arch Pathol Lab Med. 2016. PMID: 27684978 Review.
Cited by
-
Adenocarcinoma in Intraductal Tubulopapillary Neoplasm of the Pancreas: A Case Report and Literature Review.Cureus. 2023 Aug 5;15(8):e43006. doi: 10.7759/cureus.43006. eCollection 2023 Aug. Cureus. 2023. PMID: 37674950 Free PMC article.
-
Intraductal tubulopapillary neoplasm (ITPN) of the pancreas: a distinct entity among pancreatic tumors.Histopathology. 2022 Sep;81(3):297-309. doi: 10.1111/his.14698. Epub 2022 May 27. Histopathology. 2022. PMID: 35583805 Free PMC article.
-
Total Pancreatectomy with Splenectomy for Multifocal Intraductal Tubulopapillary Neoplasm (ITPN) of the Pancreas Associated with Invasive Component: Report of a Rare Case.Am J Case Rep. 2020 Jul 10;21:e924760. doi: 10.12659/AJCR.924760. Am J Case Rep. 2020. PMID: 32647104 Free PMC article.
-
Imaging findings of intraductal tubulopapillary neoplasm (ITPN) of the pancreas: Two case reports and literature review.Medicine (Baltimore). 2019 Feb;98(6):e14426. doi: 10.1097/MD.0000000000014426. Medicine (Baltimore). 2019. PMID: 30732200 Free PMC article.
-
Balloon Extraction of an Intraductal Tubulopapillary Neoplasm of the Bile Duct During Endoscopic Retrograde Cholangiopancreatography.ACG Case Rep J. 2020 Nov 24;7(11):e00481. doi: 10.14309/crj.0000000000000481. eCollection 2020 Nov. ACG Case Rep J. 2020. PMID: 33269290 Free PMC article.
References
-
- Yamaguchi H, Shimizu M, Ban S, Koyama I, Hatori T, Fujita I, Yamamoto M, Kawamura S, Kobayashi M, Ishida K, et al. Intraductal tubulopapillary neoplasms of the pancreas distinct from pancreatic intraepithelial neoplasia and intraductal papillary mucinous neoplasms. Am J Surg Pathol. 2009;33:1164–1172. doi: 10.1097/PAS.0b013e3181a162e5. - DOI - PubMed
-
- Date K, Okabayashi T, Shima Y, Iwata J, Sumiyoshi T, Kozuki A, Morita S, Hata Y, Noda Y, Nishioka A, Matsumoto M. Clinicopathological features and surgical outcomes of intraductal tubulopapillary neoplasm of the pancreas: a systematic review. Langenbeck's Arch Surg. 2016;401:439–447. doi: 10.1007/s00423-016-1391-6. - DOI - PubMed
-
- Brierley JD. TNM classification of malignant tumours: John Wiley & Sons; 2017.
-
- Basturk O, Adsay V, Askan G, Dhall D, Zamboni G, Shimizu M, Cymes K, Carneiro F, Balci S, Sigel C, et al. Intraductal tubulopapillary neoplasm of the pancreas: a clinicopathologic and immunohistochemical analysis of 33 cases. Am J Surg Pathol. 2017;41:313–325. doi: 10.1097/PAS.0000000000000782. - DOI - PMC - PubMed
-
- Del Chiaro M, Mucelli RP, Blomberg J, Segersvärd R, Verbeke C. Is intraductal tubulopapillary neoplasia a new entity in the spectrum of familial pancreatic cancer syndrome? Familial Cancer. 2014;13:227–229. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
