

Comparison of Outcomes of antibiotic Drugs and Appendectomy (CODA) trial: a protocol for the pragmatic randomised study of appendicitis treatment
- PMID: 29146633
- PMCID: PMC5695382
- DOI: 10.1136/bmjopen-2017-016117
Comparison of Outcomes of antibiotic Drugs and Appendectomy (CODA) trial: a protocol for the pragmatic randomised study of appendicitis treatment
Abstract
Introduction: Several European studies suggest that some patients with appendicitis can be treated safely with antibiotics. A portion of patients eventually undergo appendectomy within a year, with 10%-15% failing to respond in the initial period and a similar additional proportion with suspected recurrent episodes requiring appendectomy. Nearly all patients with appendicitis in the USA are still treated with surgery. A rigorous comparative effectiveness trial in the USA that is sufficiently large and pragmatic to incorporate usual variations in care and measures the patient experience is needed to determine whether antibiotics are as good as appendectomy.
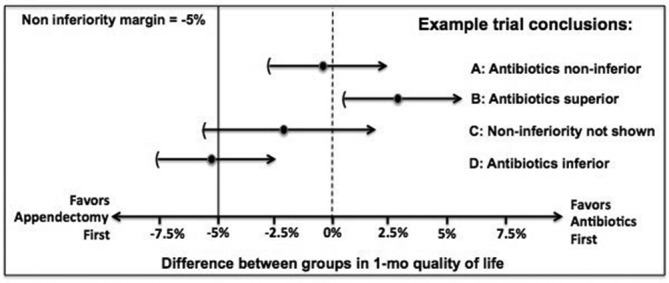
Objectives: The Comparing Outcomes of Antibiotic Drugs and Appendectomy (CODA) trial for acute appendicitis aims to determine whether the antibiotic treatment strategy is non-inferior to appendectomy.
Methods/analysis: CODA is a randomised, pragmatic non-inferiority trial that aims to recruit 1552 English-speaking and Spanish-speaking adults with imaging-confirmed appendicitis. Participants are randomised to appendectomy or 10 days of antibiotics (including an option for complete outpatient therapy). A total of 500 patients who decline randomisation but consent to follow-up will be included in a parallel observational cohort. The primary analytic outcome is quality of life (measured by the EuroQol five dimension index) at 4 weeks. Clinical adverse events, rate of eventual appendectomy, decisional regret, return to work/school, work productivity and healthcare utilisation will be compared. Planned exploratory analyses will identify subpopulations that may have a differential risk of eventual appendectomy in the antibiotic treatment arm.
Ethics and dissemination: This trial was approved by the University of Washington's Human Subjects Division. Results from this trial will be presented in international conferences and published in peer-reviewed journals.
Trial registration number: NCT02800785.
Keywords: adult surgery; appendicitis; patient-centred research; treatment options.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Coldrey E. Five years of conservative treatment of acute appendicitis. J Int Coll Surg 1959;32:255–61.
-
- Wojciechowicz KH, Hoffkamp HJ, van Hulst RA. Conservative treatment of acute appendicitis: an overview. Int Marit Health 2010;62:265–72. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases