

Service readiness of health facilities in Bangladesh, Haiti, Kenya, Malawi, Namibia, Nepal, Rwanda, Senegal, Uganda and the United Republic of Tanzania
- PMID: 29147054
- PMCID: PMC5677617
- DOI: 10.2471/BLT.17.191916
Service readiness of health facilities in Bangladesh, Haiti, Kenya, Malawi, Namibia, Nepal, Rwanda, Senegal, Uganda and the United Republic of Tanzania
Abstract
Objective: To evaluate the service readiness of health facilities in Bangladesh, Haiti, Kenya, Malawi, Namibia, Nepal, Rwanda, Senegal, Uganda and the United Republic of Tanzania.
Methods: Using existing data from service provision assessments of the health systems of the 10 study countries, we calculated a service readiness index for each of 8443 health facilities. This index represents the percentage availability of 50 items that the World Health Organization considers essential for providing health care. For our analysis we used 37-49 of the items on the list. We used linear regression to assess the independent explanatory power of four national and four facility-level characteristics on reported service readiness.
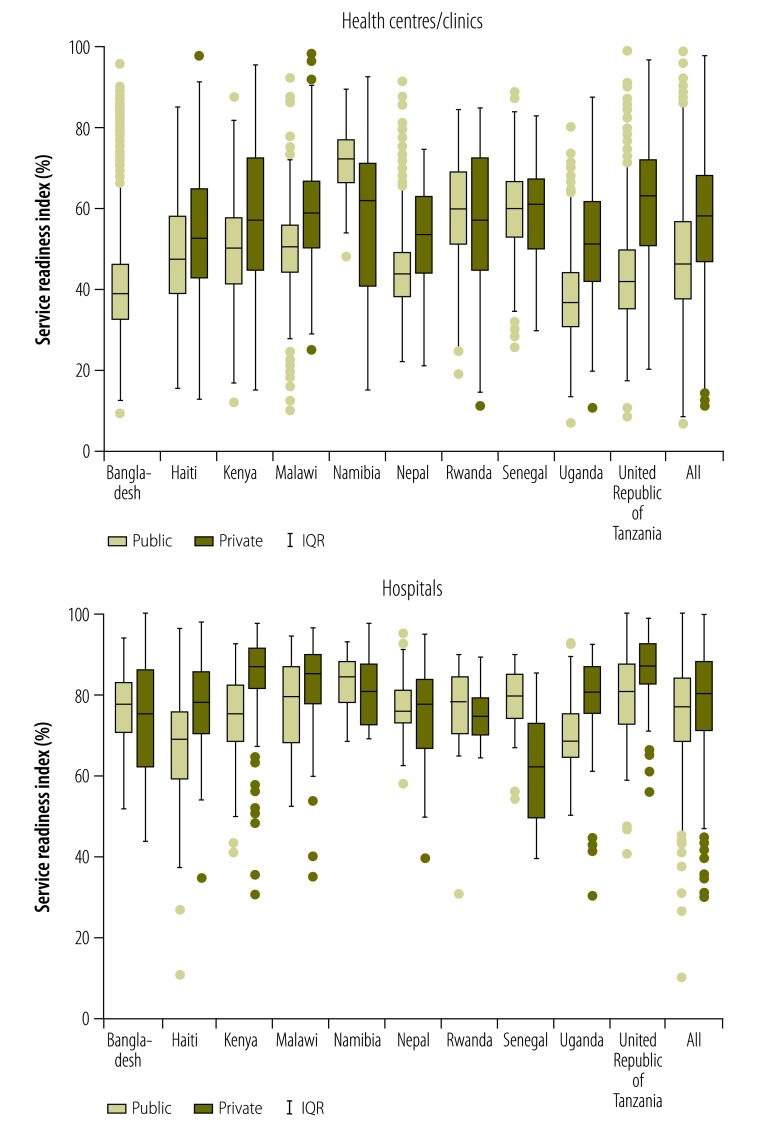
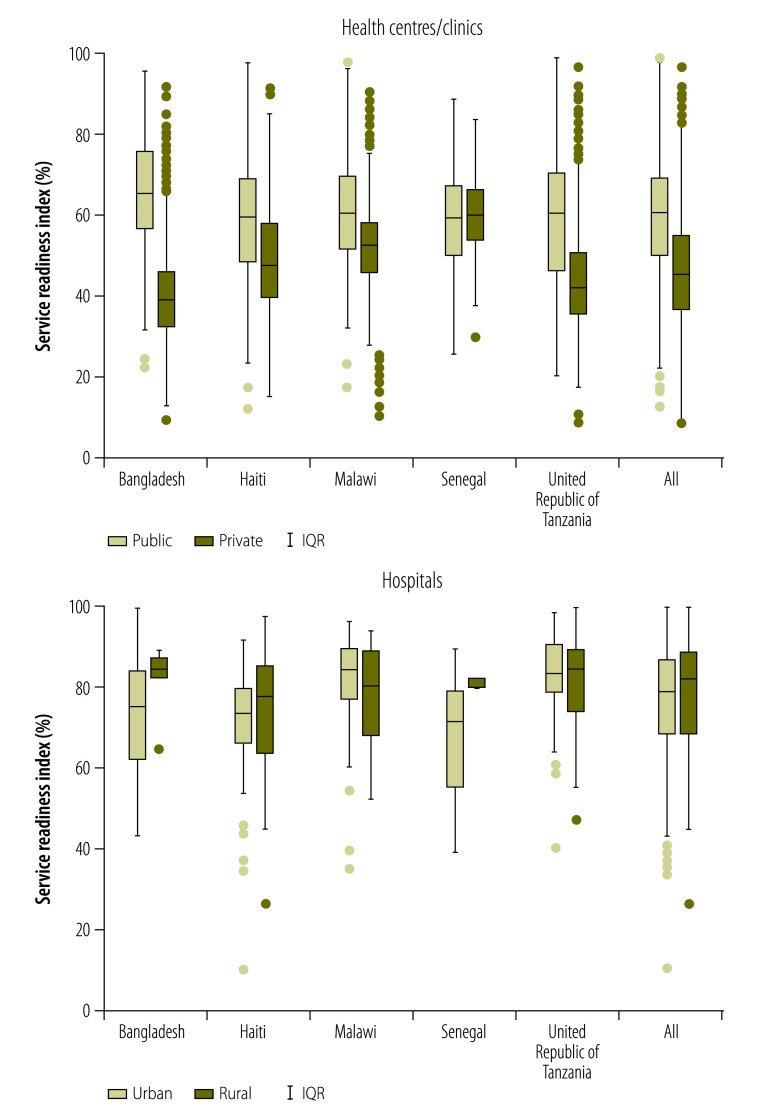
Findings: The mean values for the service readiness index were 77% for the 636 hospitals and 52% for the 7807 health centres/clinics. Deficiencies in medications and diagnostic capacity were particularly common. The readiness index varied more between hospitals and health centres/clinics in the same country than between them. There was weak correlation between national factors related to health financing and the readiness index.
Conclusion: Most health facilities in our study countries were insufficiently equipped to provide basic clinical care. If countries are to bolster health-system capacity towards achieving universal coverage, more attention needs to be given to within-country inequities.
Objectif: Évaluer la disponibilité des services dans les établissements de santé du Bangladesh, d'Haïti, du Kenya, du Malawi, de Namibie, du Népal, d'Ouganda, de République-Unie de Tanzanie, du Rwanda et du Sénégal.
Méthodes: En nous appuyant sur les données existantes tirées de l'évaluation de la prestation des services dans les systèmes de santé des 10 pays étudiés, nous avons calculé un indice de disponibilité des services pour chacun des 8443 établissements de santé. Cet indice correspond à la disponibilité en pourcentage de 50 éléments que l'Organisation mondiale de la Santé estime essentiels pour assurer les soins de santé. Dans le cadre de notre analyse, nous avons utilisé entre 37 et 49 éléments de la liste. Nous avons eu recours à une régression linéaire pour évaluer le pouvoir explicatif indépendant de quatre caractéristiques nationales et quatre caractéristiques au niveau des établissements concernant la disponibilité des services établie.
Résultats: Les valeurs moyennes de l'indice de disponibilité des services étaient de 77% pour les 636 hôpitaux et de 52% pour les 7807 centres de santé/dispensaires. L'analyse a révélé des insuffisances particulièrement courantes en matière de médicaments et de capacités de diagnostic. L'indice de disponibilité variait davantage entre les hôpitaux et les centres de santé/dispensaires d'un même pays qu'entre différents pays. Une faible corrélation a été constatée entre les facteurs nationaux liés au financement de la santé et l'indice de disponibilité.
Conclusion: La plupart des établissements de santé des pays étudiés n'étaient pas dotés d'équipements suffisants pour prodiguer les soins cliniques de base. Il est nécessaire de prêter davantage attention aux inégalités au sein des pays pour qu'ils renforcent les capacités de leur système de santé en vue d'assurer une couverture universelle.
Objetivo: Evaluar la disponibilidad del servicio de los centros sanitarios en Bangladesh, Haití, Kenya, Malawi, Namibia, Nepal, la República Unida de Tanzanía, Rwanda, Senegal y Uganda.
Métodos: Usando los datos existentes de las evaluaciones sobre prestación de servicios de sistemas sanitarios de los 10 países de estudio, se ha calculado un índice de disponibilidad del servicio para cada uno de los 8443 centros sanitarios. El índice representa el porcentaje de disponibilidad de 50 elementos que la Organización Mundial de la Salud considera esenciales para proporcionar atención sanitaria. Para el análisis, se han utilizado entre 37 y 49 de los elementos de la lista. Se ha utilizado la regresión lineal para evaluar el poder independiente descriptivo de cuatro características nacionales y cuatro a nivel del centro sobre la disponibilidad del servicio registrado.
Resultados: Los valores medios del índice de la disponibilidad del servicio fueron del 77% para los 636 hospitales y del 52% para los 7807 centros de salud/clínicas. Las deficiencias en los medicamentos y la capacidad de diagnóstico fueron particularmente comunes. El índice de disponibilidad varió más entre hospitales y centros de salud/clínicas en el mismo país que entre países. Existe una correlación débil entre los factores nacionales relacionados con la financiación sanitaria y el índice de disponibilidad.
Conclusión: La mayoría de los centros sanitarios en nuestros países de estudio fueron equipados de forma insuficiente para proporcionar atención sanitaria básica. Si los países van a reforzar la capacidad del sistema sanitario hasta conseguir la cobertura universal, se necesita poner más atención a las desigualdades dentro del país.
الغرض: تقييم جاهزية خدمات المرافق الصحية في بنغلاديش وهايتي وكينيا وملاوي وناميبيا ونيبال ورواندا والسنغال وأوغندا وجمهورية تنزانيا المتحدة.
الطريقة: باستخدام البيانات المتاحة من واقع تقييمات تقديم خدمات أنظمة الصحة في بلدان الدراسة العشرة (10)، قمنا بحساب مؤشر جاهزية الخدمة لكل من المرافق الصحية البالغ عددها 8443 مرفقًا. ويمثل هذا المؤشر نسبة التوفر المئوية لخمسين عنصرًا تعتبرها منظمة الصحة العالمية ضرورية لتوفير الرعاية الصحية. واستخدمنا 37-49 من العناصر المدرجة في القائمة لإجراء التحليل الصادر عنا. وقد استخدمنا أسلوب التحوّف الخطي لتقييم القدرة التوضيحية المستقلة لأربع خصائص وطنية وعلى مستوى المرافق الصحية فيما يتعلق بجاهزية الخدمات الواردة في التقارير.
النتائج: بلغت القيم المتوسطة لمؤشر جاهزية الخدمة 77٪ لعدد 636 مستشفى و52٪ لعدد 7807 مراكز صحية وعيادات. وكانت أوجه القصور شائعة في الأدوية والقدرة التشخيصية بوجه خاص. وظهر تباين في مؤشر الجاهزية بشكل أكبر بين المستشفيات والمراكز الصحية/العيادات الموجودة في نفس البلد أكثر مما بينها وبين مثيلاتها في البلدان الأخرى. وكان هناك ارتباط ضعيف بين العوامل الوطنية المتصلة بتمويل الصحة ومؤشر الجاهزية.
الاستنتاج: لم تكن معظم المرافق الصحية في بلدان دراستنا مجهزة تجهيزًا كافيًا لتوفير الرعاية السريرية الأساسية. وإذا ما أرادت البلدان تعزيز قدرة النظام الصحي على تحقيق التغطية الشاملة، فإنه ينبغي إيلاء مزيد من الاهتمام لحالات التفاوت داخل البلدان .
目的: 旨在评估海地、肯尼亚、卢旺达、马拉维、孟加拉国、纳米比亚、尼泊尔、塞内加尔、坦桑尼亚共和国和乌干达卫生机构服务配备状态。.
方法: 运用从这 10 个研究对象国卫生系统服务提供评估机构提供的现有数据,我们对 8443 个卫生机构的服务配备指数进行了计算。该指数代表 50 个由世界卫生组织认定的医疗保健必要项目的可用情况。 我们选取其中 37–49 个项目进行分析。我们采用线性回归法对服务配备报告上的四个国家级和四个机构级特征的独立阐释能力进行了评估。.
结果: 其中 636 家医院的服务配备指数平均数是 77%,且 7807 家医疗中心/诊所的平均数为 52%。给药和诊断能力不足尤为普遍。相同国家医院和医疗中心/诊所间的配备指数差异比不同国家间的相应配备指数差异更大。与卫生筹资相关的国家因素和配备指数之间相关性较弱。.
结论: 我们的研究对象国中,大多数国家的卫生机构在提供基本卫生护理方面配备不足。如果这些国家计划提升卫生系统能力,以实现全民卫生服务,它们需要多关注国内的不公平现象。.
Цель: Оценить степень готовности медицинских учреждений к оказанию услуг в Бангладеш, Гаити, Кении, Малави, Намибии, Непале, Объединенной Республике Танзания, Руанде, Сенегале и Уганде.
Методы: Используя имеющиеся данные, полученные из оценок предоставления медицинского обслуживания системами здравоохранения в 10 исследуемых странах, авторы рассчитали индекс готовности к оказанию услуг для каждого из 8443 медицинских учреждений. Этот индекс представляет собой процентный показатель наличия 50 пунктов, которые Всемирная организация здравоохранения считает необходимыми для оказания медицинской помощи. Для анализа авторы использовали от 37 до 49 пунктов из этого списка. Авторы использовали линейную регрессию для оценки степени влияния независимых показателей — четырех характеристик на национальном уровне и четырех характеристик на уровне медицинского учреждения — на заявленную степень готовности к оказанию услуг.
Результаты: Средние значения индекса готовности к оказанию услуг составили 77% для 636 больниц и 52% для 7807 медицинских центров и клиник. Особенно был распространен недостаток медикаментов и диагностического потенциала. Индекс готовности больше варьировался между больницами и медицинскими центрами/клиниками внутри одной страны, чем между разными странами. Наблюдалась слабая корреляция между национальными факторами, связанными с финансированием здравоохранения, и индексом готовности.
Вывод: Большинство медицинских учреждений в исследуемых странах были недостаточно подготовлены для оказания базовой клинической помощи. Если страны будут наращивать потенциал системы здравоохранения в целях обеспечения всеобщего охвата, им следует больше внимания уделять неравенству внутри страны.
Figures
References
-
- Transforming our world: the 2030 agenda for sustainable development. New York: United Nations; 2015.
-
- Millennium development goals indicators [Internet]. New York: United Nations Statistics Division; 2017. Available from: http://mdgs.un.org/unsd/mdg/default.aspx [cited 2017 Aug 16].
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical