

Modelling historical changes in the force-of-infection of Chagas disease to inform control and elimination programmes: application in Colombia
- PMID: 29147578
- PMCID: PMC5680445
- DOI: 10.1136/bmjgh-2017-000345
Modelling historical changes in the force-of-infection of Chagas disease to inform control and elimination programmes: application in Colombia
Abstract
Background: WHO's 2020 milestones for Chagas disease include having all endemic Latin American countries certified with no intradomiciliary Trypanosoma cruzi transmission, and infected patients under care. Evaluating the variation in historical exposure to infection is crucial for assessing progress and for understanding the priorities to achieve these milestones.
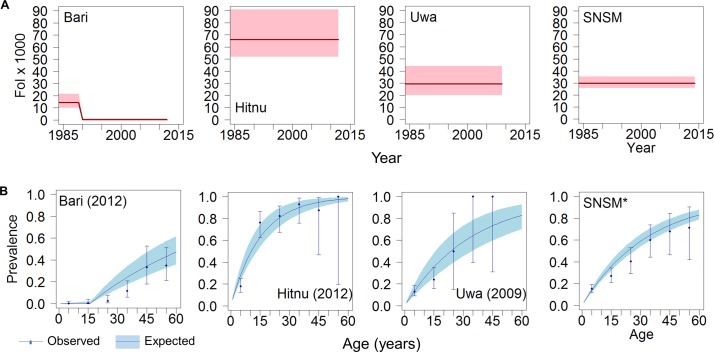
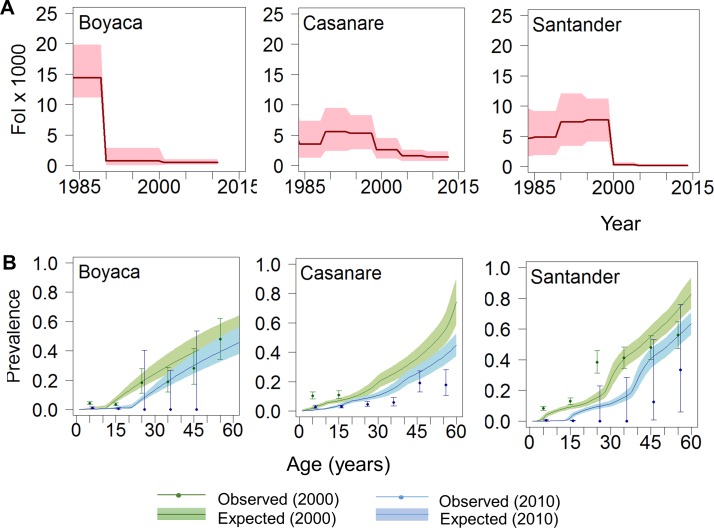
Methods: Focusing on Colombia, all the available age-structured serological surveys (undertaken between 1995 and 2014) were searched and compiled. A total of 109 serosurveys were found, comprising 83 742 individuals from rural (indigenous and non-indigenous) and urban settings in 14 (out of 32) administrative units (departments). Estimates of the force-of-infection (FoI) were obtained by fitting and comparing three catalytic models using Bayesian methods to reconstruct temporal and spatial patterns over the course of three decades (between 1984 and 2014).
Results: Significant downward changes in the FoI were identified over the course of the three decades, and in some specific locations the predicted current seroprevalence in children aged 0-5 years is <1%. However, pronounced heterogeneity exists within departments, especially between indigenous, rural and urban settings, with the former exhibiting the highest FoI (up to 66 new infections/1000 people susceptible/year). The FoI in most of the indigenous settings remain unchanged during the three decades investigated. Current prevalence in adults in these 15 departments varies between 10% and 90% depending on the dynamics of historical exposure.
Conclusions: Assessing progress towards the control of Chagas disease requires quantifying the impact of historical exposure on current age-specific prevalence at subnational level. In Colombia, despite the evident progress, there is a marked heterogeneity indicating that in some areas the vector control interventions have not been effective, hindering the possibility of achieving interruption by 2020. A substantial burden of chronic cases remains even in locations where serological criteria for transmission interruption may have been achieved, therefore still demanding diagnosis and treatment interventions.
Keywords: chagas disease; control strategies; cross-sectional survey; mathematical modelling; serology.
Conflict of interest statement
Competing interests: None declared.
Figures




References
-
- World health organization. Chagas disease in Latin America: an epidemiological update based on 2010 estimates. Wkly Epidemiol Rec 2015;90:33–43 http://www.ncbi.nlm.nih.gov/pubmed/25671846 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources