

Stimuli-Responsive Delivery of Therapeutics for Diabetes Treatment
- PMID: 29147685
- PMCID: PMC5685194
- DOI: 10.1002/btm2.10036
Stimuli-Responsive Delivery of Therapeutics for Diabetes Treatment
Abstract
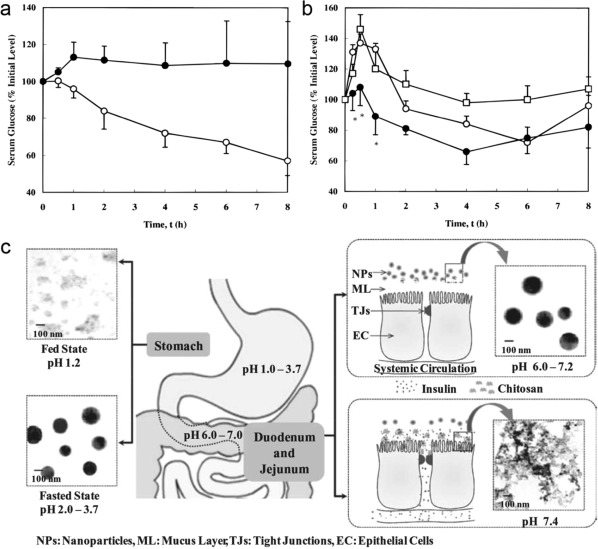
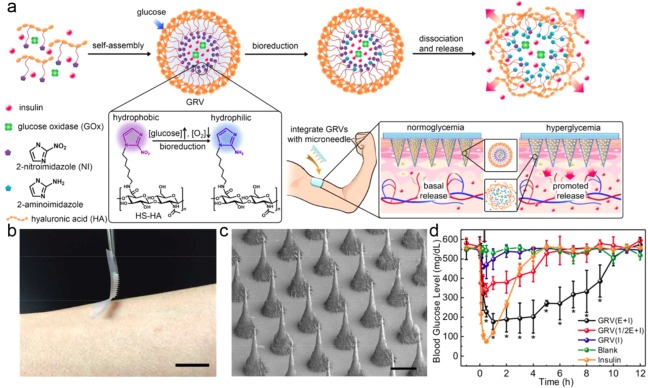
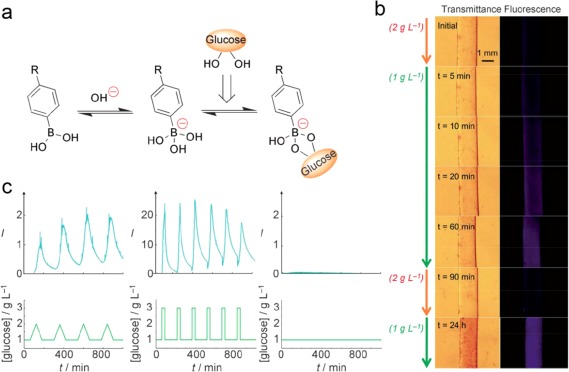
Diabetic therapeutics, including insulin and glucagon-like peptide 1 (GLP-1), are essential for diabetic patients to regulate blood glucose levels. However, conventional treatments that are based on subcutaneous injections are often associated with poor glucose control and a lack of patient compliance. In this review, we focus on the different stimuli-responsive systems to deliver therapeutics for diabetes treatment to improve patient comfort and prevent complications. Specifically, the pH-responsive systems for oral drug delivery are introduced first. Then, the closed-loop glucose-responsive systems are summarized based on different glucose-responsive moieties, including glucose oxidase (GOx), glucose binding protein (GBP), and phenylboronic acid (PBA). Finally, the on-demand delivery systems activated by external remote triggers are also discussed. We conclude by discussing advantages and limitations of current strategies, as well as future opportunities and challenges in this area.
Keywords: diabetes; drug delivery; insulin; stimuli-responsive.
Figures
References
-
- Atkinson MA, Eisenbarth GS. Type 1 diabetes: new perspectives on disease pathogenesis and treatment. Lancet. 2001;358:221–229. - PubMed
-
- Stumvoll M, Goldstein BJ, van Haeften TW. Type 2 diabetes: principles of pathogenesis and therapy. Lancet. 2005;365:1333–1346. - PubMed
-
- International Diabetes Federation. 4/20/2016. http://www.idf.org.
-
- American Diabetes Association . 4/20/2016. http://www.diabetes.org.
-
- Lieberman SM, DiLorenzo TP. A comprehensive guide to antibody and T‐cell responses in type 1 diabetes. Tissue Antigens. 2003;62:359–377. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
