

Non-invasive methods for estimating mPAP in COPD using cardiovascular magnetic resonance imaging
- PMID: 29147768
- PMCID: PMC5834560
- DOI: 10.1007/s00330-017-5143-y
Non-invasive methods for estimating mPAP in COPD using cardiovascular magnetic resonance imaging
Abstract
Purpose: Pulmonary hypertension (PH) is associated with a poor outcome in chronic obstructive pulmonary disease (COPD) and is diagnosed invasively. We aimed to assess the diagnostic accuracy and prognostic value of non-invasive cardiovascular magnetic resonance (CMR) models.
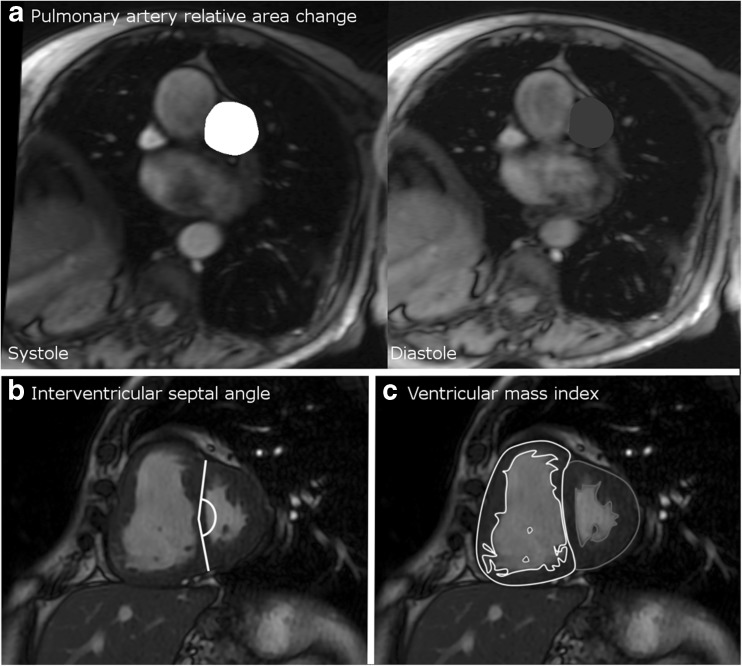
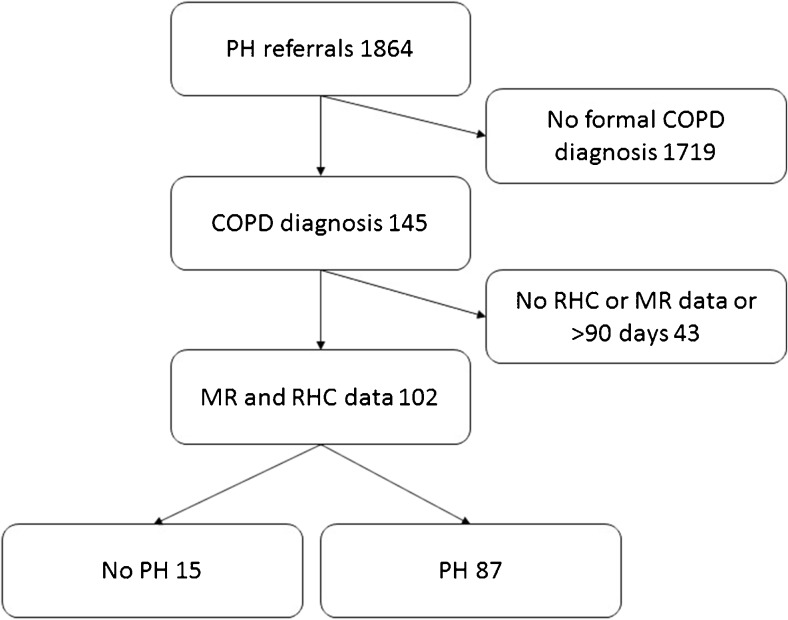
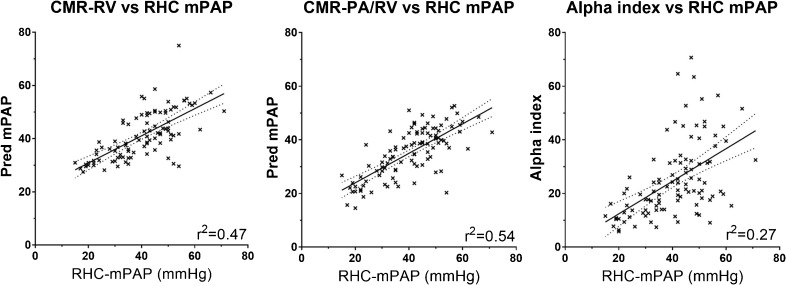
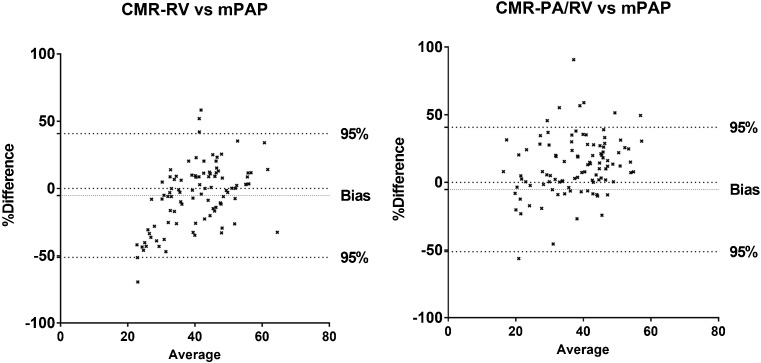
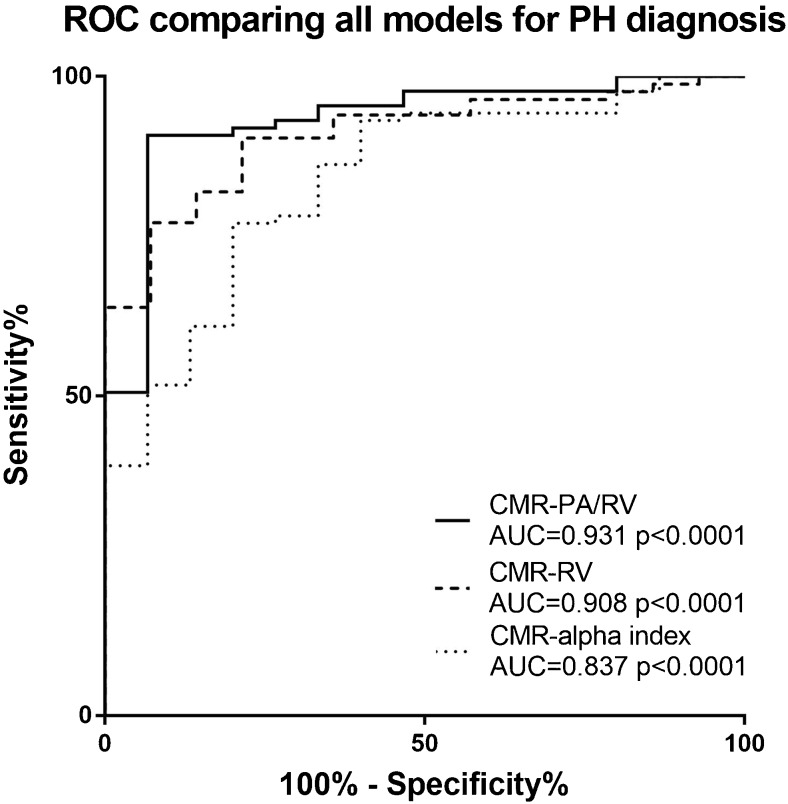
Methods: Patients with COPD and suspected PH, who underwent CMR and right heart catheter (RHC) were identified. Three candidate models were assessed: 1, CMR-RV model, based on right ventricular (RV) mass and interventricular septal angle; 2, CMR PA/RV includes RV mass, septal angle and pulmonary artery (PA) measurements; 3, the Alpha index, based on RV ejection fraction and PA size.
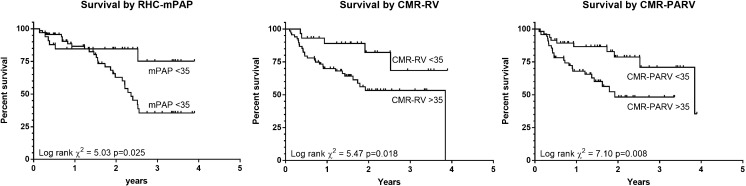
Results: Of 102 COPD patients, 87 had PH. The CMR-PA/RV model had the strongest diagnostic accuracy (sensitivity 92%, specificity 80%, positive predictive value 96% and negative predictive value 63%, AUC 0.93, p<0.0001). Splitting RHC-mPAP, CMR-RV and CMR-PA/RV models by 35mmHg gave a significant difference in survival, with log-rank chi-squared 5.03, 5.47 and 7.10. RV mass and PA relative area change were the independent predictors of mortality at multivariate Cox regression (p=0.002 and 0.030).
Conclusion: CMR provides diagnostic and prognostic information in PH-COPD. The CMR-PA/RV model is useful for diagnosis, the RV mass index and PA relative area change are useful to assess prognosis.
Key points: • Pulmonary hypertension is a marker of poor outcome in COPD. • MRI can predict invasively measured mean pulmonary artery pressure. • Cardiac MRI allows for estimation of survival in COPD. • Cardiac MRI may be useful for follow up or future trials. • MRI is potentially useful to assess pulmonary hypertension in patients with COPD.
Keywords: Cardiac; Chronic Obstructive Pulmonary Disease; Cor Pulmonale; Magnetic Resonance Imaging; Pulmonary Hypertension.
Conflict of interest statement
Guarantor
The scientific guarantor of this publication is Dr Andrew Swift.
Conflict of interest
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Funding
This work was supported by NIHR grant NIHR-RP-R3-12-027, Wellcome grant 205188/Z/16/Z and MRC grant MR/M008894/1. The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health. D. Capener was part funded by an unrestricted research grant from Bayer.
Statistics and biometry
No complex statistical methods were necessary for this paper.
Informed consent
Written informed consent was waived by the Institutional Review Board.
Ethical approval
Institutional Review Board approval was obtained.
Methodology
• retrospective
• diagnostic or prognostic study
• performed at one institution
Figures
Similar articles
-
Noninvasive estimation of PA pressure, flow, and resistance with CMR imaging: derivation and prospective validation study from the ASPIRE registry.JACC Cardiovasc Imaging. 2013 Oct;6(10):1036-1047. doi: 10.1016/j.jcmg.2013.01.013. Epub 2013 Jun 13. JACC Cardiovasc Imaging. 2013. PMID: 23769494
-
Diagnostic accuracy of cardiovascular magnetic resonance imaging of right ventricular morphology and function in the assessment of suspected pulmonary hypertension results from the ASPIRE registry.J Cardiovasc Magn Reson. 2012 Jun 21;14(1):40. doi: 10.1186/1532-429X-14-40. J Cardiovasc Magn Reson. 2012. PMID: 22720870 Free PMC article.
-
Assessment of right ventricle-to-pulmonary artery coupling by three-dimensional echocardiography in pre-capillary pulmonary hypertension: comparison with tricuspid annular plane systolic excursion /systolic pulmonary artery pressure ratio.BMC Med Imaging. 2025 Apr 3;25(1):108. doi: 10.1186/s12880-025-01650-z. BMC Med Imaging. 2025. PMID: 40181260 Free PMC article.
-
Methods for Evaluating Right Ventricular Function and Ventricular-Arterial Coupling.Prog Cardiovasc Dis. 2016 Jul-Aug;59(1):42-51. doi: 10.1016/j.pcad.2016.06.001. Epub 2016 Jul 5. Prog Cardiovasc Dis. 2016. PMID: 27393072 Review.
-
Quantitative magnetic resonance imaging of pulmonary hypertension: a practical approach to the current state of the art.J Thorac Imaging. 2014 Mar;29(2):68-79. doi: 10.1097/RTI.0000000000000079. J Thorac Imaging. 2014. PMID: 24552882 Free PMC article. Review.
Cited by
-
GOLD COPD DOCUMENT 2023: a brief update for practicing cardiologists.Clin Res Cardiol. 2024 Feb;113(2):195-204. doi: 10.1007/s00392-023-02217-0. Epub 2023 May 26. Clin Res Cardiol. 2024. PMID: 37233751 Free PMC article. Review.
-
Updated Perspectives on Pulmonary Hypertension in COPD.Int J Chron Obstruct Pulmon Dis. 2020 Jun 9;15:1315-1324. doi: 10.2147/COPD.S211841. eCollection 2020. Int J Chron Obstruct Pulmon Dis. 2020. PMID: 32606641 Free PMC article. Review.
-
Right main pulmonary artery distensibility on dynamic ventilation CT and its association with respiratory function.Eur Radiol Exp. 2024 Apr 4;8(1):50. doi: 10.1186/s41747-024-00441-5. Eur Radiol Exp. 2024. PMID: 38570418 Free PMC article.
-
Predicting pulmonary hemodynamics in pediatric pulmonary arterial hypertension using cardiac magnetic resonance imaging and machine learning: an exploratory pilot study.Int J Cardiovasc Imaging. 2025 Jun 14. doi: 10.1007/s10554-025-03434-6. Online ahead of print. Int J Cardiovasc Imaging. 2025. PMID: 40515976
-
Combined automated 3D volumetry by pulmonary CT angiography and echocardiography for detection of pulmonary hypertension.Eur Radiol. 2019 Nov;29(11):6059-6068. doi: 10.1007/s00330-019-06188-7. Epub 2019 Apr 8. Eur Radiol. 2019. PMID: 30963276
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
