

Single-cell heterogeneity in ductal carcinoma in situ of breast
- PMID: 29148540
- PMCID: PMC6192037
- DOI: 10.1038/modpathol.2017.143
Single-cell heterogeneity in ductal carcinoma in situ of breast
Abstract
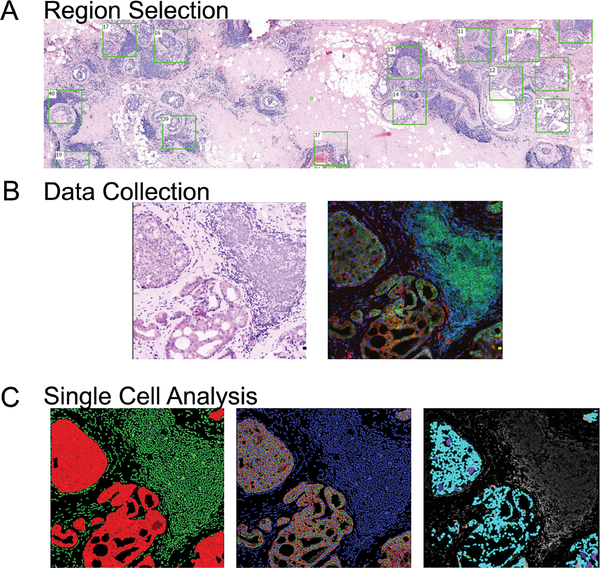
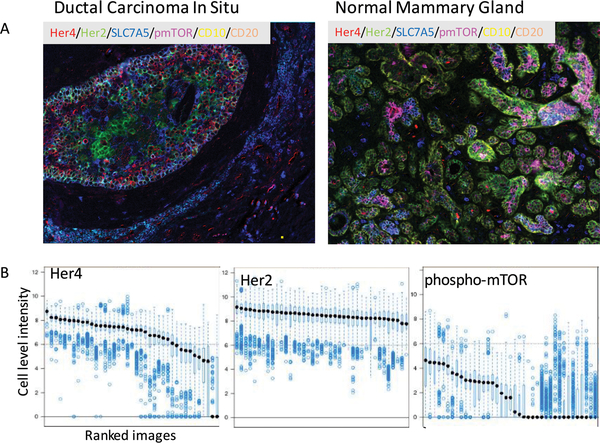
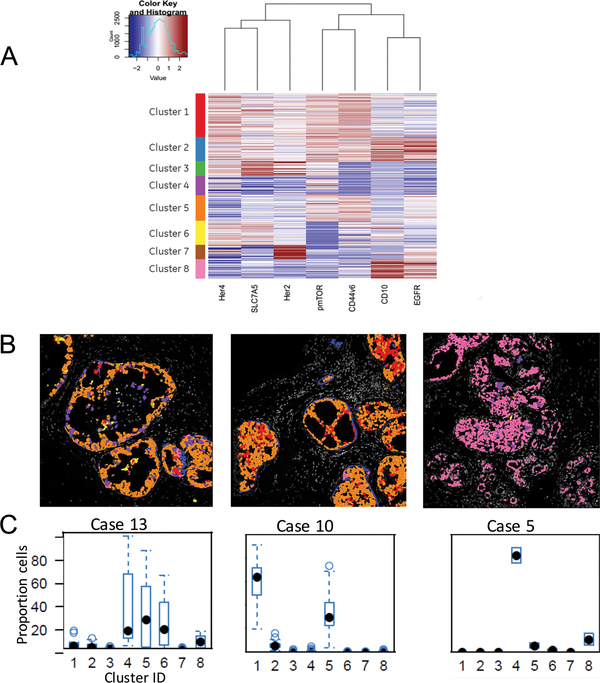
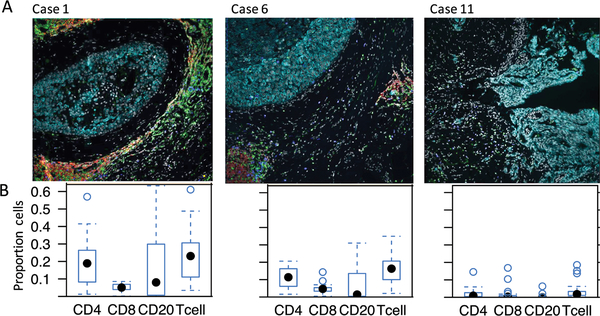
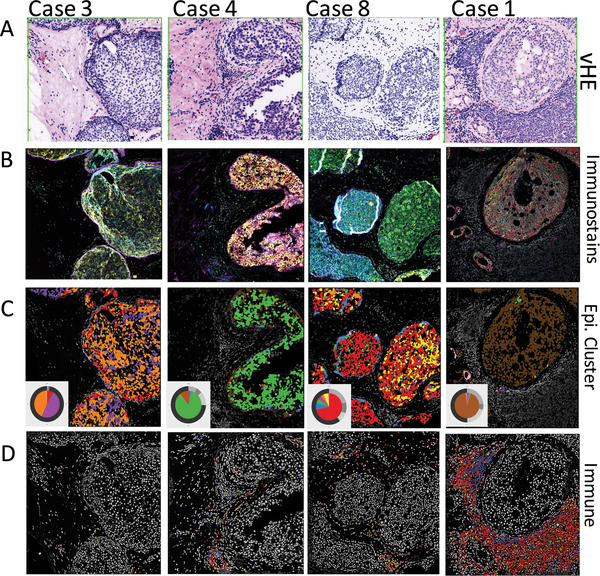
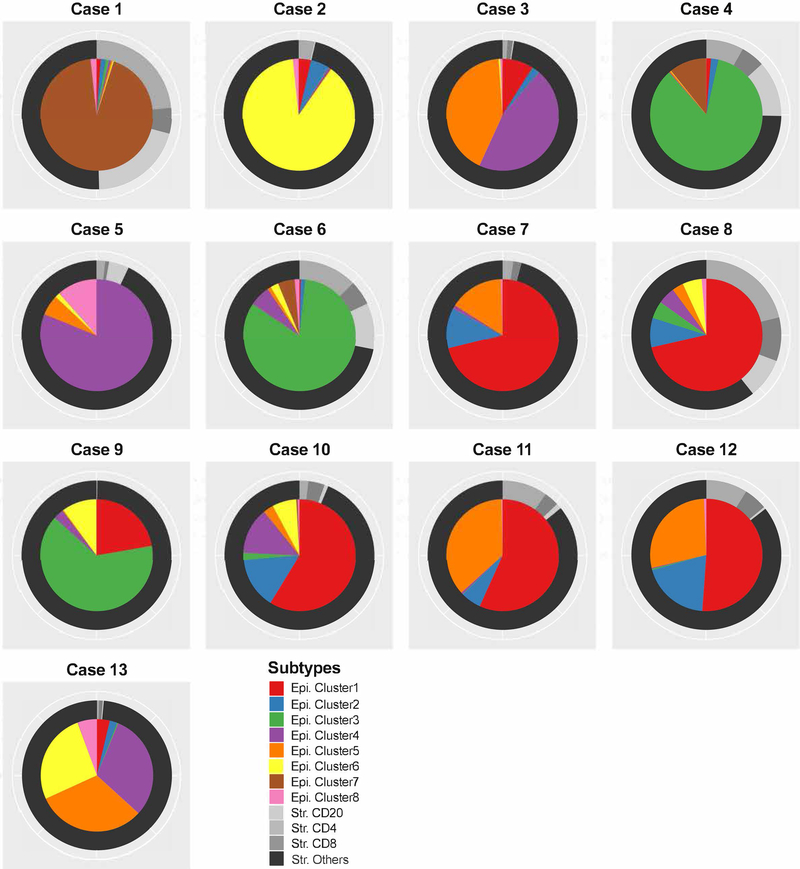
Heterogeneous patterns of mutations and RNA expression have been well documented in invasive cancers. However, technological challenges have limited the ability to study heterogeneity of protein expression. This is particularly true for pre-invasive lesions such as ductal carcinoma in situ of the breast. Cell-level heterogeneity in ductal carcinoma in situ was analyzed in a single 5 μm tissue section using a multiplexed immunofluorescence analysis of 11 disease-related markers (EGFR, HER2, HER4, S6, pmTOR, CD44v6, SLC7A5 and CD10, CD4, CD8 and CD20, plus pan-cytokeratin, pan-cadherin, DAPI, and Na+K+ATPase for cell segmentation). Expression was quantified at cell level using a single-cell segmentation algorithm. K-means clustering was used to determine co-expression patterns of epithelial cell markers and immune markers. We document for the first time the presence of epithelial cell heterogeneity within ducts, between ducts and between patients with ductal carcinoma in situ. There was moderate heterogeneity in a distribution of eight clusters within each duct (average Shannon index 0.76; range 0-1.61). Furthermore, within each patient, the average Shannon index across all ducts ranged from 0.33 to 1.02 (s.d. 0.09-0.38). As the distribution of clusters within ducts was uneven, the analysis of eight ducts might be sufficient to represent all the clusters ie within- and between-duct heterogeneity. The pattern of epithelial cell clustering was associated with the presence and type of immune infiltrates, indicating a complex interaction between the epithelial tumor and immune system for each patient. This analysis also provides the first evidence that simultaneous analysis of both the epithelial and immune/stromal components might be necessary to understand the complex milieu in ductal carcinoma in situ lesions.
Figures
References
-
- Cancer Govindan R.. Attack of the clones. Science. 2014:169–70. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
