

Robust optimization in IMPT using quadratic objective functions to account for the minimum MU constraint
- PMID: 29148570
- PMCID: PMC5774242
- DOI: 10.1002/mp.12677
Robust optimization in IMPT using quadratic objective functions to account for the minimum MU constraint
Abstract
Purpose: Currently, in clinical practice of intensity-modulated proton therapy (IMPT), the influence of the minimum monitor unit (MU) constraint is taken into account through postprocessing after the optimization is completed. This may degrade the plan quality and plan robustness. This study aims to mitigate the impact of the minimum MU constraint directly during the plan robust optimization.
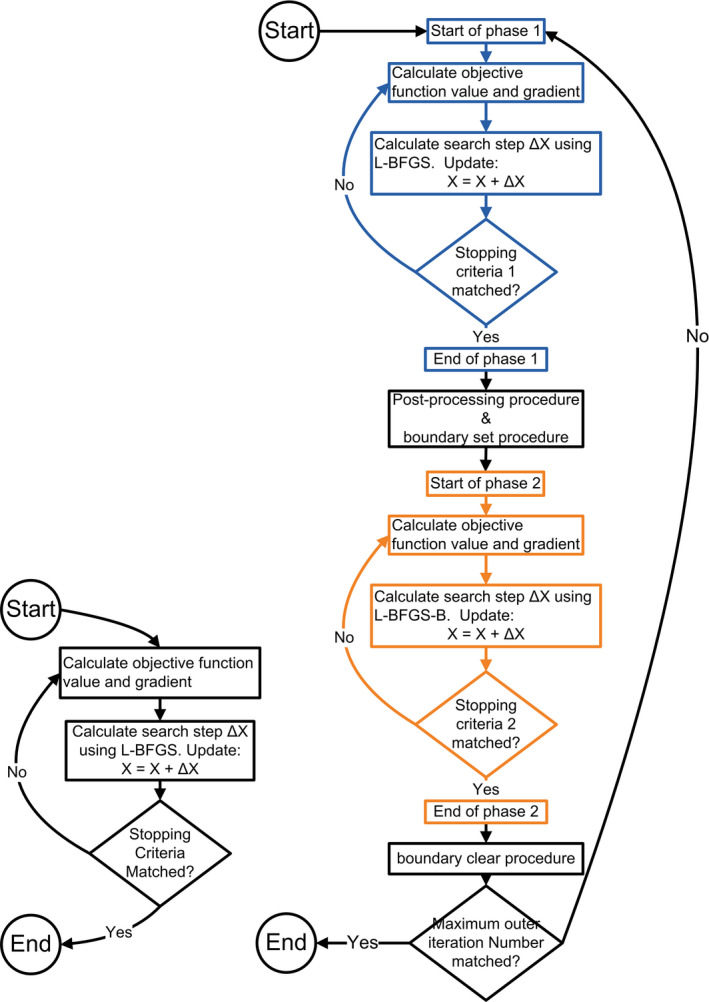
Methods and materials: Cao et al. have demonstrated a two-stage method to account for the minimum MU constraint using linear programming without the impact of uncertainties considered. In this study, we took the minimum MU constraint into consideration using quadratic optimization and simultaneously had the impact of uncertainties considered using robust optimization. We evaluated our method using seven cancer patients with different machine settings.
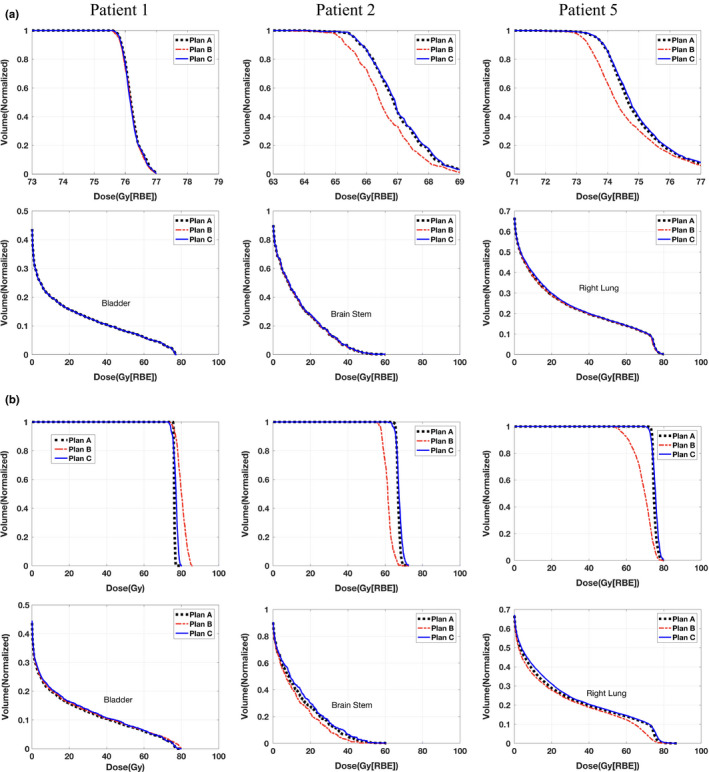
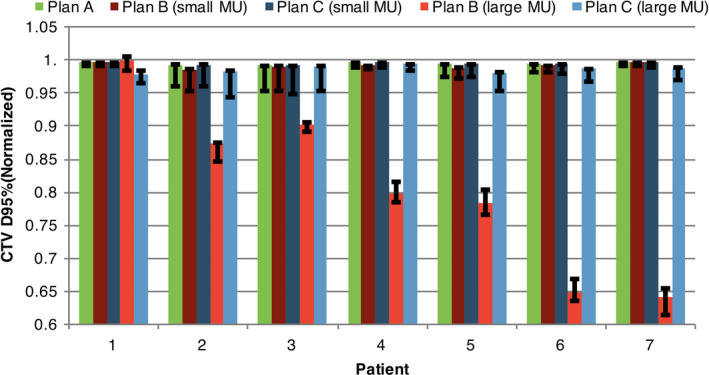
Result: The new method achieved better plan quality than the conventional method. The D95% of the clinical target volume (CTV) normalized to the prescription dose was (mean [min-max]): (99.4% [99.2%-99.6%]) vs. (99.2% [98.6%-99.6%]). Plan robustness derived from these two methods was comparable. For all seven patients, the CTV dose-volume histogram band gap (narrower band gap means more robust plans) at D95% normalized to the prescription dose was (mean [min-max]): (1.5% [0.5%-4.3%]) vs. (1.2% [0.6%-3.8%]).
Conclusion: Our new method of incorporating the minimum MU constraint directly into the plan robust optimization can produce machine-deliverable plans with better tumor coverage while maintaining high-plan robustness.
Keywords: L-BFGS-B; deliverable robustness; intensity-modulated proton therapy (IMPT); minimum MU constraint; quadratic optimization.
© 2017 American Association of Physicists in Medicine.
Conflict of interest statement
The authors have no relevant conflicts of interest to disclose.
Figures
References
-
- Stuschke M, Kaiser A, Pottgen C, Lubcke W, Farr J. Potentials of robust intensity modulated scanning proton plans for locally advanced lung cancer in comparison to intensity modulated photon plans. Radiother Oncol. 2012;104:45–51. - PubMed
-
- Sejpal S, Komaki R, Tsao A, et al. Early findings on toxicity of proton beam therapy with concurrent chemotherapy for nonsmall cell lung cancer. Cancer. 2011;117:3004–3013. - PubMed
-
- Lomax A. Intensity modulation methods for proton radiotherapy. Phys Med Biol. 1999;44:185. - PubMed
-
- Lomax AJ. Habilitation Thesis, ETH; 2004.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
