

Key bottlenecks to the provision of safe obstetric anaesthesia in low- income countries; a cross-sectional survey of 64 hospitals in Uganda
- PMID: 29149877
- PMCID: PMC5693492
- DOI: 10.1186/s12884-017-1566-3
Key bottlenecks to the provision of safe obstetric anaesthesia in low- income countries; a cross-sectional survey of 64 hospitals in Uganda
Abstract
Background: Despite recent advances in surgery and anaesthesia which significantly improve safety, many health facilities in low-and middle-income countries (LMICs) remain chronically under-resourced with inability to cope effectively with serious obstetric complications (Knight et al., PLoS One 8:e63846, 2013). As a result many of these countries still have unacceptably high maternal and neonatal mortality rates. Recent data at the national referral hospitals in East Africa reported that none of the national referral hospitals met the World Federation of Societies of Anesthesiologists (WFSA) international standards required to provide safe obstetric anaesthesia (Epiu I: Challenges of Anesthesia in Low-and Middle-Income Countries. WFSA; 2014 http://wfsa.newsweaver.com/Newsletter/p8c8ta4ri7a1wsacct9y3u?a=2&p=47730565&t=27996496 ). In spite of this evidence, factors contributing to maternal mortality related to anaesthesia in LMICs and the magnitude of these issues have not been comprehensively studied. We therefore set out to assess regional referral, district, private for profit and private not-for profit hospitals in Uganda.
Methods: We conducted a cross-sectional survey at 64 government and private hospitals in Uganda using pre-set questionnaires to the anaesthetists and hospital directors. Access to the minimum requirements for safe obstetric anaesthesia according to WFSA guidelines were also checked using a checklist for operating and recovery rooms.
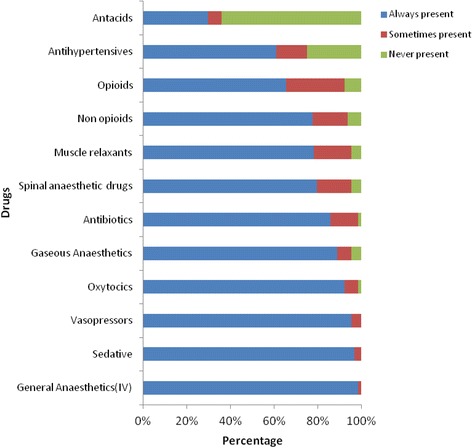
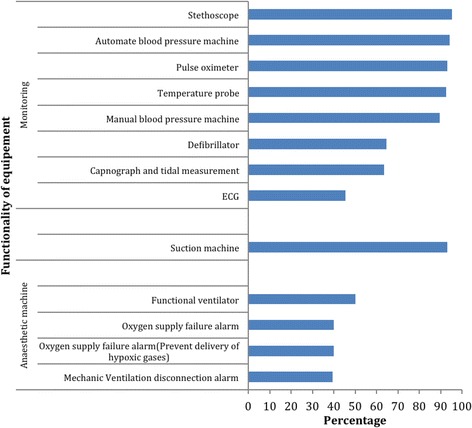
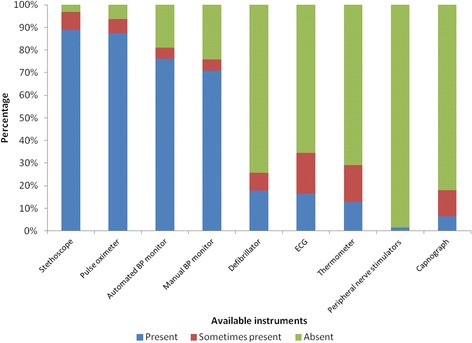
Results: Response rate was 100% following personal interviews of anaesthetists, and hospital directors. Only 3 of the 64 (5%) of the hospitals had all requirements available to meet the WFSA International guidelines for safe anaesthesia. Additionally, 54/64 (84%) did not have a trained physician anaesthetist and 5/64 (8%) had no trained providers for anaesthesia at all. Frequent shortages of drugs were reported for regional/neuroaxial anaesthesia, and other essential drugs were often lacking such as antacids and antihypertensives. We noted that many of the anaesthesia machines present were obsolete models without functional safety alarms and/or mechanical ventilators. Continuous ECG was only available in 3/64 (5%) of hospitals.
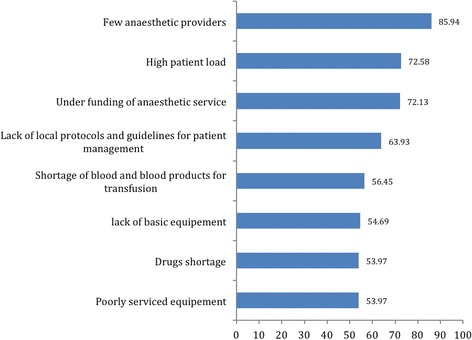
Conclusion: We conclude that there is a significant lack of essential equipment for the delivery of safe anaesthesia across this region. This is compounded by the shortage of trained providers and inadequate supervision. It is therefore essential to strengthen anaesthesia services by addressing these specific deficiencies. This will include improved training of associate clinicians, training more physician anaesthetists and providing the basic equipment required to provide safe and effective care. These services are key components of comprehensive emergency obstetric care and anaesthetists are crucial in managing critically ill mothers and ensuring good surgical outcomes.
Keywords: Caesarean section; Health system; Low-income countries; Maternal mortality; Obstetric Anaesthesia; Quality; Safe Anaesthesia; Universal health care.
Conflict of interest statement
Ethics approval and consent to participate
Ethical approval was obtained from Makerere University School of Medicine Research and Ethics Committee (SOMREC), P. O. Box 7072 Kampala, Uganda. +256,414,530,020.
The Uganda National Council for Science & Technology Ethics Committee (UNCST), P. O. Box 6448 Kampala, Uganda +256,414,705,500.
Consent to participate in the study was obtained form participants.
Consent for publication
Not Applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Weiser TG, Regenbogen SE, Thompson KD, Haynes AB, Lipsitz SR, Berry WR, Gawande AA. An estimation of the global volume of surgery: a modelling strategy based on available data. Lancet. 372(9633):139–44. - PubMed
-
- Keenan RL BC. Decreasing frequency of anesthetic cardiac arrests. J Clin Anesth. 1991;3:354–7. - PubMed
-
- Moller JT JN, Espersen K, Ravlo O, Pedersen BD, Jensen PF RN, Rasmussen LS, Pedersen T, Cooper JB, Gravenstein JS, Chraemmer Jorgensen B DM, Wiberg Jorgensen F, Heslet L, Johansen SH. Randomized evaluation of pulse oximetry in 20,802 patients. II. Perioperative events and postoperative complications. Anesthesiology. 1993;78:444–53. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
