

Review
doi: 10.1053/j.semdp.2017.11.002.
Epub 2017 Nov 3.
Non-neoplastic histiocytic and dendritic cell disorders in lymph nodes
Affiliations
- PMID: 29150219
- PMCID: PMC5803315
- DOI: 10.1053/j.semdp.2017.11.002
Item in Clipboard
Review
Non-neoplastic histiocytic and dendritic cell disorders in lymph nodes
Semin Diagn Pathol.
2018 Jan.
Abstract
Benign and malignant proliferations of histiocytes and dendritic cells may be encountered in lymph nodes. Reactive histiocytic and dendritic cell infiltrates occur in response to diverse stimuli and in addition to causing lymphadenopathy, may be present unexpectedly in lymph nodes excised for other indications. This review summarizes the pathogenesis and histopathological features of the various non-neoplastic histiocytic and dendritic cell infiltrates that can occur in lymph nodes.
Published by Elsevier Inc.
Figures
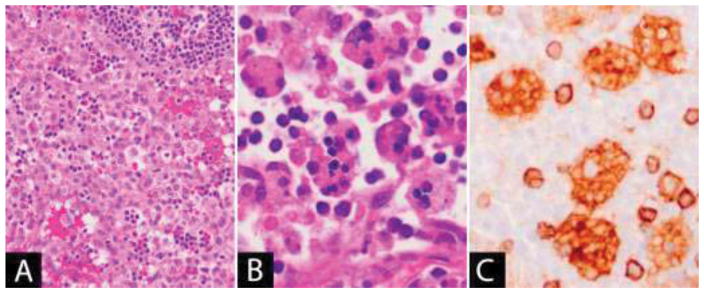
Lymph node sinuses are dilated and filled with benign-appearing histiocytes. (B–C) Hemophagocytic lymphohistiocytosis: (B) Histiocytes in the lymph node sinuses show prominent hemophagocytosis, (C) which can be highlighted using histiocytic markers (CD4 in image).
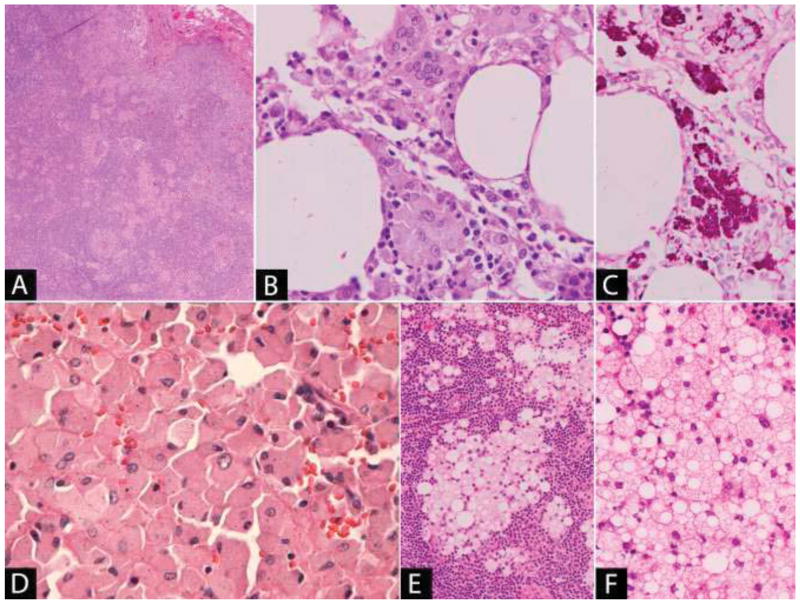
(A) Small aggregates of macrophages are present in the lymph node sinuses and in the parenchyma forming loose epithelioid granulomas. (B) The macrophages have eosinophilic granular cytoplasm and occasional multinucleated giant cells are present. (C) The bacilli are positive with DPAS stain. (D) Histiocytosis following joint replacement: Sheets of polygonal histiocytes with abundant eosinophilic cytoplasm containing small black particles consistent with metal wear debris. (E–F) Silicone lymphadenopathy due to breast implant: (E) Aggregates of macrophages with abundant foamy, vacuolar cytoplasm are present within the lymph node. (F) The vacuoles are colorless and the silicone, where present, has a refractile quality and is non-polarizable.
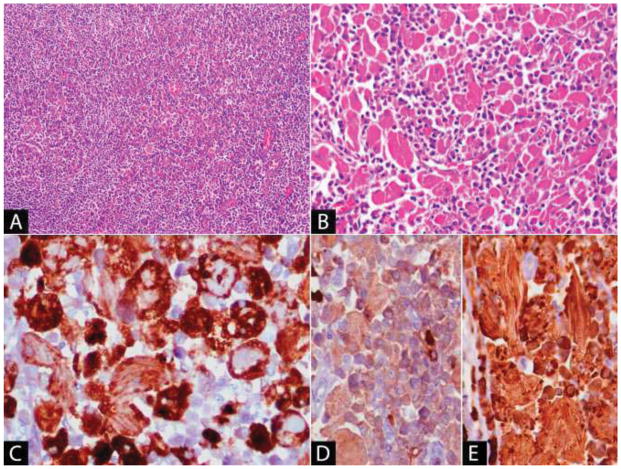
(A) The lymphoma component is diffuse in areas, containing only scattered admixed histiocytes. (B) Elsewhere, there are sheets of histiocytes with abundant eosinophilic fibrillary cytoplasm. (C) The histiocytes are positive with CD68, which aids in visualizing the intracytoplasmic rhomboid and needle-shaped crystals. Immunohistochemistry for kappa (D) and lambda (E) show that the crystals and background plasma cells in this case are positive for lambda light chain.
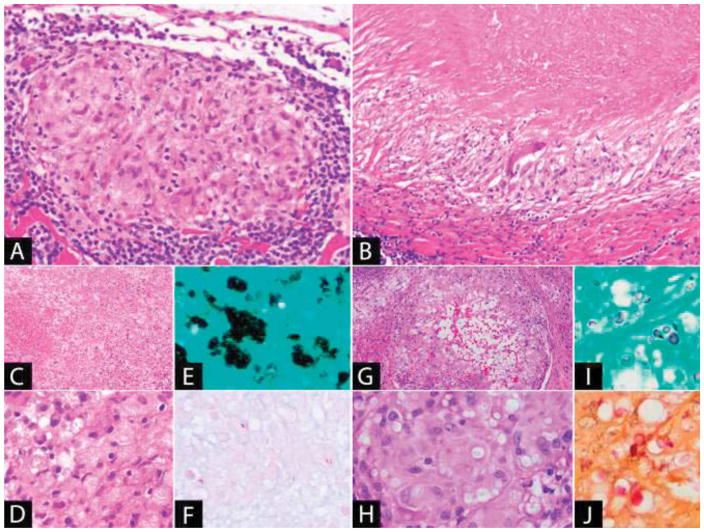
(A) Non-necrotizing granuloma: The granuloma is well-demarcated and composed of epithelioid histiocytes with a peripheral lymphoid cuff. (B) Necrotizing granuloma: There is a large area of necrosis surrounded by a peripheral rim of epithelioid histiocytes. A giant cell is also present. (C–E) Disseminated histoplasmosis: (C) The lymph node is effaced by sheets of macrophages with extensive necrosis. (D) The yeast is present in clusters within the cytoplasm of the macrophages and is positive with (E) GMS stain. (F) Acid-fast bacilli (Fite): Mycobacteria, a cause of necrotizing granulomatous lymphadenitis, may be few in number and difficult to identify. (G–J): Cryptococcal lymphadenitis: (G) Granulomatous inflammation with central cystic spaces. (H) The yeast is visible within the cytoplasm of the histiocytes as faintly staining structures within clear spaces. It is positive with (I) GMS and (J) mucicarmine stains.
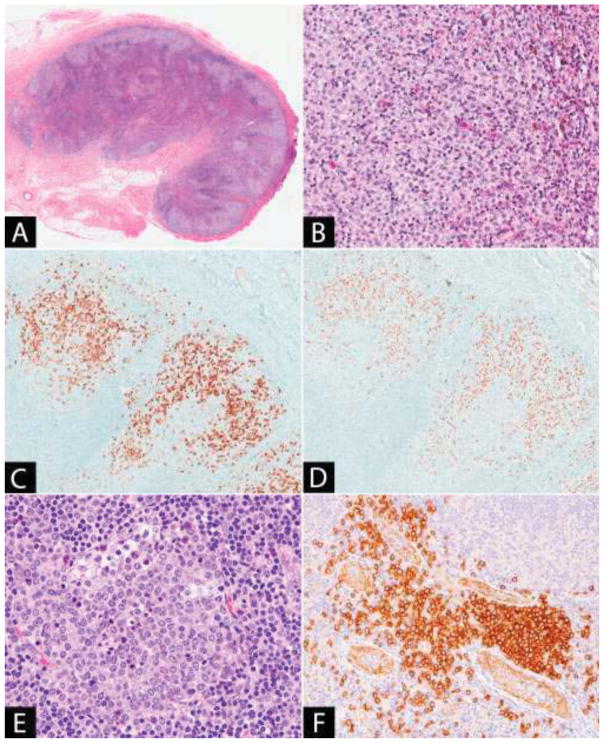
(A) The lymph node paracortex is expanded by pale staining nodules. (B) The pale staining areas are composed of an admixture of dendritic cells, Langerhans cells and histiocytes, some of which contain pigment. The Langerhans cells may be numerous and are identified by immunohistochemistry with (C) CD1a and (D) langerin. (E–F) Plasmacytoid dendritic cell aggregate: (E) The plasmacytoid dendritic cells have pale cytoplasm and fine chromatin. Scattered tingible body macrophages are present. (F) CD123 stains both the plasmacytoid dendritic cells and the endothelial cells, highlighting the location of the plasmacytoid dendritic cell aggregate adjacent to the high endothelial venules.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
