

Urgent versus post-stabilisation antiretroviral treatment in hospitalised HIV-infected children in Kenya (PUSH): a randomised controlled trial
- PMID: 29150377
- PMCID: PMC5777310
- DOI: 10.1016/S2352-3018(17)30167-4
Urgent versus post-stabilisation antiretroviral treatment in hospitalised HIV-infected children in Kenya (PUSH): a randomised controlled trial
Abstract
Background: Urgent antiretroviral therapy (ART) among hospitalised HIV-infected children might accelerate recovery or worsen outcomes associated with immune reconstitution. We aimed to compare urgent versus post-stabilisation ART among hospitalised HIV-infected children in Kenya.
Methods: In this unmasked randomised controlled trial, we randomly assigned (1:1) HIV-infected, ART-naive children aged 0-12 years who were eligible for treatment to receive ART within 48 h (urgent group) or in 7-14 days (post-stabilisation group) at four hospitals in Kenya (two in Nairobi and two in western Kenya). We excluded children with suspected or confirmed CNS infection. A statistician not involved in study procedures did block randomisation with variable block sizes generated using STATA version 12. We followed children for 6 months for primary outcomes: mortality, drug toxicity, and immune reconstitution inflammatory syndrome (IRIS). We did all analyses in a modified intention-to-treat population. This trial is registered with ClinicalTrials.gov, number NCT02063880.
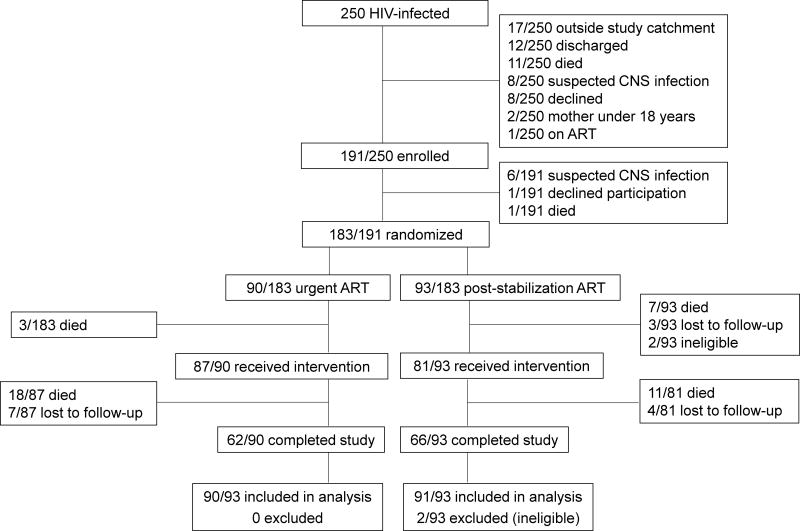
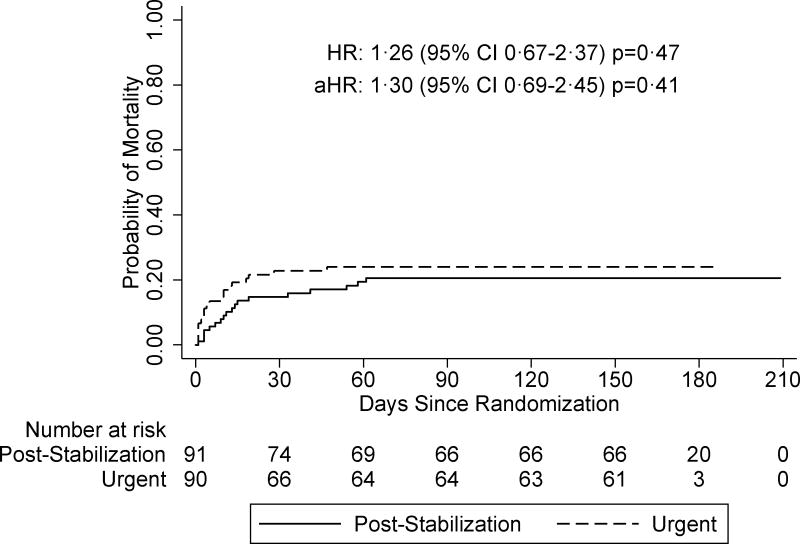
Findings: We began enrolment on April 24, 2013, and completed follow-up on Nov 17, 2015. We enrolled 191 (76%) of 250 hospitalised HIV-infected children. Of these, 183 children were randomly assigned: 90 to urgent ART and 93 to post-stabilisation ART. 181 (99%) of 183 children were included in the modified intention-to-treat analysis. Median age was 1·9 years (IQR 0·8-4·8). Baseline sociodemographic, clinical, and virological characteristics did not differ between groups except median CD4 cell percentage, which was lower in the urgent group (13% [IQR 9-18] vs 17% [IQR 9-24]; p=0·052). Of 181 admission diagnoses, 118 (65%) were pneumonia, 58 (32%) malnutrition, and 27 (15%) suspected tuberculosis. Median time to ART was 1 day (IQR 1-1) in the urgent group and 8 days (IQR 7-11) in the post-stabilisation group. Overall, mortality risk at 6 months was 61 per 100 person-years. Mortality risk did not differ by group (70 per 100 person-years in the urgent group vs 54 per 100 person-years in the post-stabilisation group; hazard ratio [HR] 1·26, 95% CI 0·67-2·37) p=0.47, even after adjusting for baseline CD4 cell percentage (adjusted HR 1·30, 95% CI 0·69-2·45; p=0·41). The incidence of IRIS, and drug toxicity was not significantly different between trial arms. There were no differences between treatment groups in the proportion of grade 3 or 4 adverse events (34 [38%] of 90 children in the urgent group vs 40 [44%] of 91 children in the post-stabilisation group; p=0·40) or the proportion of any change in ART regimen (five [7%] vs six [8%]; p=0·79). We discontinued randomisation at interim review when the futility boundary was crossed.
Interpretation: Early mortality risk was extremely high among hospitalised HIV-infected children. Urgent ART did not improve survival.
Funding: National Institute of Child Health and Human Development, National Institutes of Health, USA.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Dr. Richardson reports grants from NIH, during the conduct of the study; personal fees from Tobira Therapeutics, Inc, personal fees from Theratechnologies, Inc., outside the submitted work. Joshua Stern reports grants from CFAR, during the conduct of the study; personal fees from University of Washington, outside the submitted work. Dr. John-Stewart reports grants from NIH, non-financial support from UW, during the conduct of the study; grants from NIH, grants from CDC, grants from Thrasher Foundation, other from UpToDate, personal fees from IMPAACT, other from NIH, outside the submitted work. Other authors have no conflicts of interest to disclose. LMC reports grants from NIH, American Academy of Pediatrics, and American Pediatric Society during the conduct of the study; grants from Firland foundation, Seattle Children’s Center for Clinical and Translational Research and Emory Univerity pediatric Research Center, outside the submitted work.
Comment in
-
Timing of antiretroviral therapy in children with advanced HIV.Lancet HIV. 2018 Jan;5(1):e2-e3. doi: 10.1016/S2352-3018(17)30193-5. Epub 2017 Nov 14. Lancet HIV. 2018. PMID: 29150376 No abstract available.
References
-
- Wagner A, Slyker J, Langat A, Inwani I, Adhiambo J, Benki-Nugent S, et al. High mortality in HIV-infected children diagnosed in hospital underscores need for faster diagnostic turnaround time in prevention of mother-to-child transmission of HIV (PMTCT) programs. BMC Pediatr. 2015;15:10. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
