

Prevalence and recognition of obesity and its associated comorbidities: cross-sectional analysis of electronic health record data from a large US integrated health system
- PMID: 29150468
- PMCID: PMC5702021
- DOI: 10.1136/bmjopen-2017-017583
Prevalence and recognition of obesity and its associated comorbidities: cross-sectional analysis of electronic health record data from a large US integrated health system
Abstract
Objective: To determine the prevalence of obesity and its related comorbidities among patients being actively managed at a US academic medical centre, and to examine the frequency of a formal diagnosis of obesity, via International Classification of Diseases, Ninth Revision (ICD-9) documentation among patients with body mass index (BMI) ≥30 kg/m2.
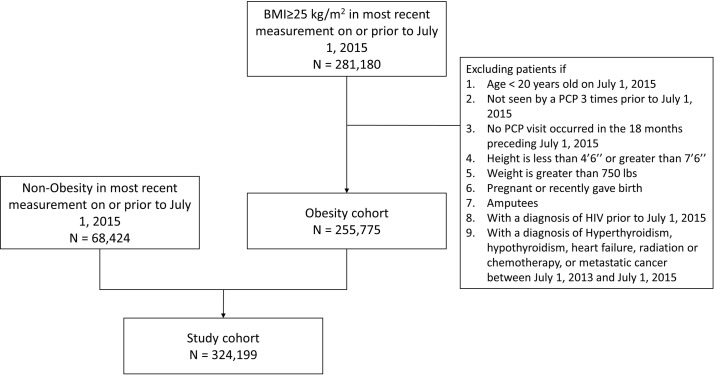
Design: The electronic health record system at Cleveland Clinic was used to create a cross-sectional summary of actively managed patients meeting minimum primary care physician visit frequency requirements. Eligible patients were stratified by BMI categories, based on most recent weight and median of all recorded heights obtained on or before the index date of 1July 2015. Relationships between patient characteristics and BMI categories were tested.
Setting: A large US integrated health system.
Results: A total of 324 199 active patients with a recorded BMI were identified. There were 121 287 (37.4%) patients found to be overweight (BMI ≥25 and <29.9), 75 199 (23.2%) had BMI 30-34.9, 34 152 (10.5%) had BMI 35-39.9 and 25 137 (7.8%) had BMI ≥40. There was a higher prevalence of type 2 diabetes, pre-diabetes, hypertension and cardiovascular disease (P value<0.0001) within higher BMI compared with lower BMI categories. In patients with a BMI >30 (n=134 488), only 48% (64 056) had documentation of an obesity ICD-9 code. In those patients with a BMI >40, only 75% had an obesity ICD-9 code.
Conclusions: This cross-sectional summary from a large US integrated health system found that three out of every four patients had overweight or obesity based on BMI. Patients within higher BMI categories had a higher prevalence of comorbidities. Less than half of patients who were identified as having obesity according to BMI received a formal diagnosis via ICD-9 documentation. The disease of obesity is very prevalent yet underdiagnosed in our clinics. The under diagnosing of obesity may serve as an important barrier to treatment initiation.
Keywords: body mass index; diagnosis; electronic health records; integrated delivery system; obesity.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: KMP reports receiving research funding from Novo Nordisk and Merck, receiving consulting fees from Novo Nordisk, and Merck, and receiving honoraria from Merck, AstraZeneca, Sanofi and Novo Nordisk for speaking/educational activities within the past 12 months. RSZ reports receiving research funding from Novo Nordisk and Merck, and receiving speaker honoraria from Merck, and received consulting fees from Novo Nordisk and Merck within the past 12 months. BJW, MWK, AM, KMC and JMB. report receiving research funding from Novo Nordisk and Merck within the past 12 months. ADM received research support from the Merck Investigator Studies Program and the Agency for Healthcare Research and Quality K08 HS024128. JB and BS were employees at Novo Nordisk and owned company stock while the research was being conducted. TMH, SXK and WW are employees of Novo Nordisk and own company stock. BB reports receiving consulting fees and research support from Novo Nordisk in the past 12 months.
Figures
References
-
- Ogden CL, Carroll MD, Fryar CD, et al. . Prevalence of obesity among adults and youth: United States, 2011-2014. NCHS Data Brief 2015:1–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical