

Disparities in Management of Cardiovascular Disease in Rural South Africa: Data From the HAALSI Study (Health and Aging in Africa: Longitudinal Studies of International Network for the Demographic Evaluation of Populations and Their Health Communities)
- PMID: 29150535
- PMCID: PMC5777525
- DOI: 10.1161/CIRCOUTCOMES.117.004094
Disparities in Management of Cardiovascular Disease in Rural South Africa: Data From the HAALSI Study (Health and Aging in Africa: Longitudinal Studies of International Network for the Demographic Evaluation of Populations and Their Health Communities)
Abstract
Background: Optimal secondary prevention is critical for the reduction of repeated cardiovascular events, and the control of cardiovascular risk factors in this context is essential. Data on secondary prevention of cardiovascular disease (CVD) in sub-Saharan Africa are needed to inform intervention strategies with a particular focus on local disparities. The aim of this study was to assess CVD management in a rural community in northeast South Africa.
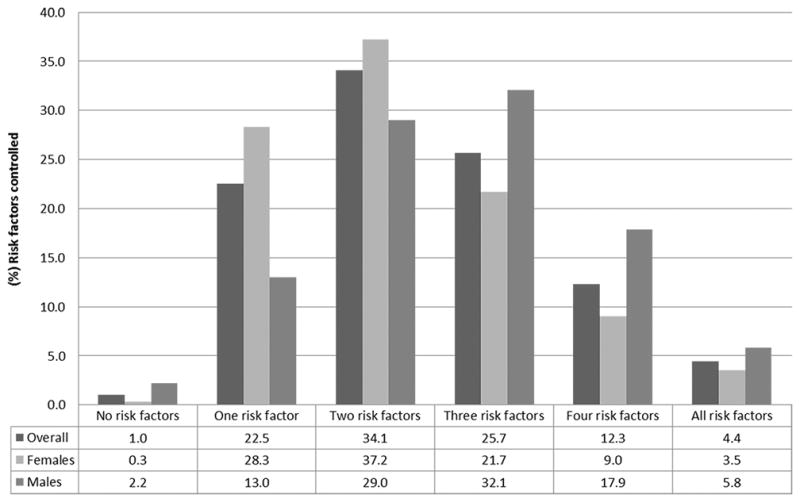
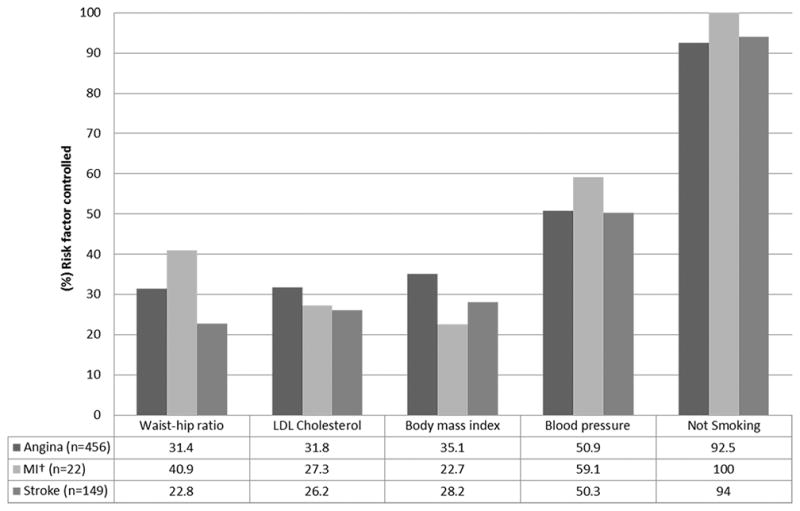
Methods and results: We recruited adults aged ≥40 years residing in the Agincourt subdistrict of Mpumalanga province. Data collection included socioeconomic and clinical data, anthropometric measures, blood pressure, human immunodeficiency virus status, and point-of-care glucose and lipid levels. CVD was defined as self-report of myocardial infarction and stroke or angina diagnosed by Rose Criteria. A linear regression model was built to identify variables independently associated with the number of cardiovascular risk factors controlled. Of 5059 subjects, 592 (11.7%) met CVD diagnostic criteria. Angina was reported in 77.0% of these subjects, stroke in 25.2%, and myocardial infarction in 3.7%. Percent controlled of the 5 individual risk factors assessed were as follows: tobacco 92.9%; blood pressure 51.2%; body mass index 33.8%; low-density lipoprotein 31.4%; and waist-to-hip ratio 29.7%. Only 4.4% had all 5 risk factors controlled and 42.4% had ≥3 risk factors controlled. Male sex (β coefficient=0.44; 95% confidence interval, 0.25-0.63; P<0.001), absence of physical disability (β coefficient=0.40; 95% confidence interval, 0.16-0.65; P=0.001), and socioeconomic status (β coefficient=0.10; 95% confidence interval, 0.01-0.19; P=0.035) were directly associated with the number of risk factors controlled.
Conclusions: Currently, CVD is not being optimally managed in this rural area of South Africa. There are significant disparities in control of CVD risk factors by sex, socioeconomic status, and level of disability. Efforts to improve secondary prevention in this population should be focused on females, subjects from lower socioeconomic status, and those with physical disabilities.
Keywords: South Africa; aging; body mass index; cardiovascular diseases; secondary prevention.
© 2017 American Heart Association, Inc.
Figures
Similar articles
-
Cardiovascular Disease Profile of the Oldest Adults in Rural South Africa: Data from the HAALSI Study (Health and Aging in Africa: Longitudinal Studies of INDEPTH Communities).J Am Geriatr Soc. 2018 Nov;66(11):2151-2157. doi: 10.1111/jgs.15567. Epub 2018 Oct 12. J Am Geriatr Soc. 2018. PMID: 30312474 Free PMC article.
-
Cardiometabolic risk in a population of older adults with multiple co-morbidities in rural south africa: the HAALSI (Health and Aging in Africa: longitudinal studies of INDEPTH communities) study.BMC Public Health. 2017 Feb 17;17(1):206. doi: 10.1186/s12889-017-4117-y. BMC Public Health. 2017. PMID: 28212629 Free PMC article.
-
Awareness, treatment, and control of dyslipidemia in rural South Africa: The HAALSI (Health and Aging in Africa: A Longitudinal Study of an INDEPTH Community in South Africa) study.PLoS One. 2017 Oct 27;12(10):e0187347. doi: 10.1371/journal.pone.0187347. eCollection 2017. PLoS One. 2017. PMID: 29077762 Free PMC article.
-
The emergence of cardiovascular disease during urbanisation of Africans.Public Health Nutr. 2002 Feb;5(1A):239-43. doi: 10.1079/phn2001299. Public Health Nutr. 2002. PMID: 12027290 Review.
-
Mediterranean-style diet for the primary and secondary prevention of cardiovascular disease.Cochrane Database Syst Rev. 2019 Mar 13;3(3):CD009825. doi: 10.1002/14651858.CD009825.pub3. Cochrane Database Syst Rev. 2019. PMID: 30864165 Free PMC article.
Cited by
-
Cardiovascular Disease Profile of the Oldest Adults in Rural South Africa: Data from the HAALSI Study (Health and Aging in Africa: Longitudinal Studies of INDEPTH Communities).J Am Geriatr Soc. 2018 Nov;66(11):2151-2157. doi: 10.1111/jgs.15567. Epub 2018 Oct 12. J Am Geriatr Soc. 2018. PMID: 30312474 Free PMC article.
-
Prevalence of and Risk Factors for Peripheral Artery Disease in Rural South Africa: A Cross-Sectional Analysis of the HAALSI Cohort.J Am Heart Assoc. 2024 Jan 2;13(1):e031780. doi: 10.1161/JAHA.123.031780. Epub 2023 Dec 29. J Am Heart Assoc. 2024. PMID: 38156447 Free PMC article.
-
World Heart Federation Roadmap for Secondary Prevention of Cardiovascular Disease: 2023 Update.Glob Heart. 2024 Jan 22;19(1):8. doi: 10.5334/gh.1278. eCollection 2024. Glob Heart. 2024. PMID: 38273995 Free PMC article.
-
Community-based care models for arterial hypertension management in non-pregnant adults in sub-Saharan Africa: a literature scoping review and framework for designing chronic services.BMC Public Health. 2022 Jun 4;22(1):1126. doi: 10.1186/s12889-022-13467-4. BMC Public Health. 2022. PMID: 35658850 Free PMC article.
-
Cardiovascular risk among community members in three communities in the Cape Metropole of the Western Cape.Afr J Prim Health Care Fam Med. 2024 May 14;16(1):e1-e7. doi: 10.4102/phcfm.v16i1.4246. Afr J Prim Health Care Fam Med. 2024. PMID: 38832373 Free PMC article.
References
-
- Sampson UKA, Amuyunzu-Nyamongo M, Mensah GA. Health Promotion and Cardiovascular Disease Prevention in Sub-Saharan Africa. Progress in Cardiovascular Diseases. 2013;56:344–355. - PubMed
-
- Madu EC, Richardson KD, Ozigbo OH, Baugh DS. Improving cardiovascular disease prevention and management in Africa: issues to consider for the 21st century. Ethn Dis. 2003;13:S71–6. - PubMed
-
- Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, AlMazroa MA, Amann M, Anderson HR, Andrews KG, Aryee M, Atkinson C, Bacchus LJ, Bahalim AN, Balakrishnan K, Balmes J, Barker-Collo S, Baxter A, Bell ML, Blore JD, Blyth F, Bonner C, Borges G, Bourne R, Boussinesq M, Brauer M, Brooks P, Bruce NG, Brunekreef B, Bryan-Hancock C, Bucello C, Buchbinder R, Bull F, Burnett RT, Byers TE, Calabria B, Carapetis J, Carnahan E, Chafe Z, Charlson F, Chen H, Chen JS, Cheng AT-A, Child JC, Cohen A, Colson KE, Cowie BC, Darby S, Darling S, Davis A, Degenhardt L, Dentener F, Des Jarlais DC, Devries K, Dherani M, Ding EL, Dorsey ER, Driscoll T, Edmond K, Ali SE, Engell RE, Erwin PJ, Fahimi S, Falder G, Farzadfar F, Ferrari A, Finucane MM, Flaxman S, Fowkes FGR, Freedman G, Freeman MK, Gakidou E, Ghosh S, Giovannucci E, Gmel G, Graham K, Grainger R, Grant B, Gunnell D, Gutierrez HR, Hall W, Hoek HW, Hogan A, Hosgood HD, III, Hoy D, Hu H, Hubbell BJ, Hutchings SJ, Ibeanusi SE, Jacklyn GL, Jasrasaria R, Jonas JB, Kan H, Kanis JA, Kassebaum N, Kawakami N, Khang Y-H, Khatibzadeh S, Khoo J-P, Kok C, Laden F, Lalloo R, Lan Q, Lathlean T, Leasher JL, Leigh J, Li Y, Lin JK, Lipshultz SE, London S, Lozano R, Lu Y, Mak J, Malekzadeh R, Mallinger L, Marcenes W, March L, Marks R, Martin R, McGale P, McGrath J, Mehta S, Memish ZA, Mensah GA, Merriman TR, Micha R, Michaud C, Mishra V, Hanafiah KM, Mokdad AA, Morawska L, Mozaffarian D, Murphy T, Naghavi M, Neal B, Nelson PK, Nolla JM, Norman R, Olives C, Omer SB, Orchard J, Osborne R, Ostro B, Page A, Pandey KD, Parry CDH, Passmore E, Patra J, Pearce N, Pelizzari PM, Petzold M, Phillips MR, Pope D, Pope CA, III, Powles J, Rao M, Razavi H, Rehfuess EA, Rehm JT, Ritz B, Rivara FP, Roberts T, Robinson C, Rodriguez-Portales JA, Romieu I, Room R, Rosenfeld LC, Roy A, Rushton L, Salomon JA, Sampson U, Sanchez-Riera L, Sanman E, Sapkota A, Seedat S, Shi P, Shield K, Shivakoti R, Singh GM, Sleet DA, Smith E, Smith KR, Stapelberg NJC, Steenland K, Stöckl H, Stovner LJ, Straif K, Straney L, Thurston GD, Tran JH, Van Dingenen R, van Donkelaar A, Veerman JL, Vijayakumar L, Weintraub R, Weissman MM, White RA, Whiteford H, Wiersma ST, Wilkinson JD, Williams HC, Williams W, Wilson N, Woolf AD, Yip P, Zielinski JM, Lopez AD, Murray CJL, Ezzati M. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. The Lancet. 2012;380:2224–2260. - PMC - PubMed
-
- Alwan A. Global status report on noncommunicable diseases 2010. Geneva: World Health Organization; 2011.
-
- Smith SC, Benjamin EJ, Bonow RO, Braun LT, Creager MA, Franklin BA, Gibbons RJ, Grundy SM, Hiratzka LF, Jones DW, Lloyd-Jones DM, Minissian M, Mosca L, Peterson ED, Sacco RL, Spertus J, Stein JH, Taubert KA. AHA/ACCF Secondary Prevention and Risk Reduction Therapy for Patients With Coronary and Other Atherosclerotic Vascular Disease: 2011 Update. Circulation. 2011;124:2458. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
