

Computed Tomography Perfusion is a Useful Adjunct to Computed Tomography Angiography in the Diagnosis of Brain Death
- PMID: 29150710
- PMCID: PMC6394546
- DOI: 10.1007/s00062-017-0631-7
Computed Tomography Perfusion is a Useful Adjunct to Computed Tomography Angiography in the Diagnosis of Brain Death
Abstract
Background: In the diagnosis of brain death (BD), computed tomography angiography (CTA) results in some cases show intracranial filling, leading to diagnostic confusion. Because cerebral circulatory arrest commences at the capillary level, we hypothesized that computed tomography perfusion (CTP) would be a more sensitive approach than CTA; therefore, the aim of the study was to compare the sensitivities of CTP and CTA in the diagnosis of BD.
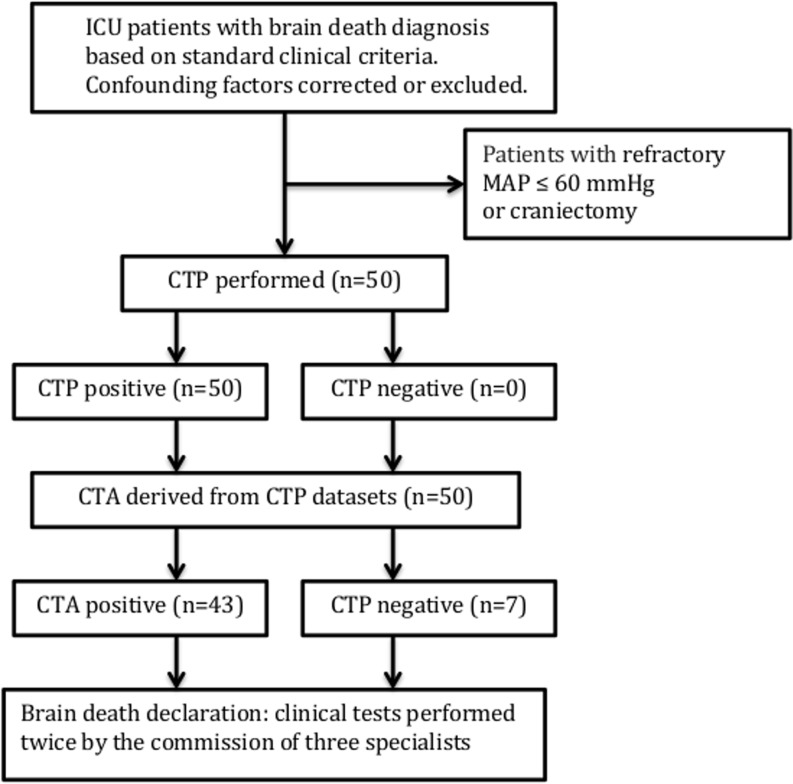
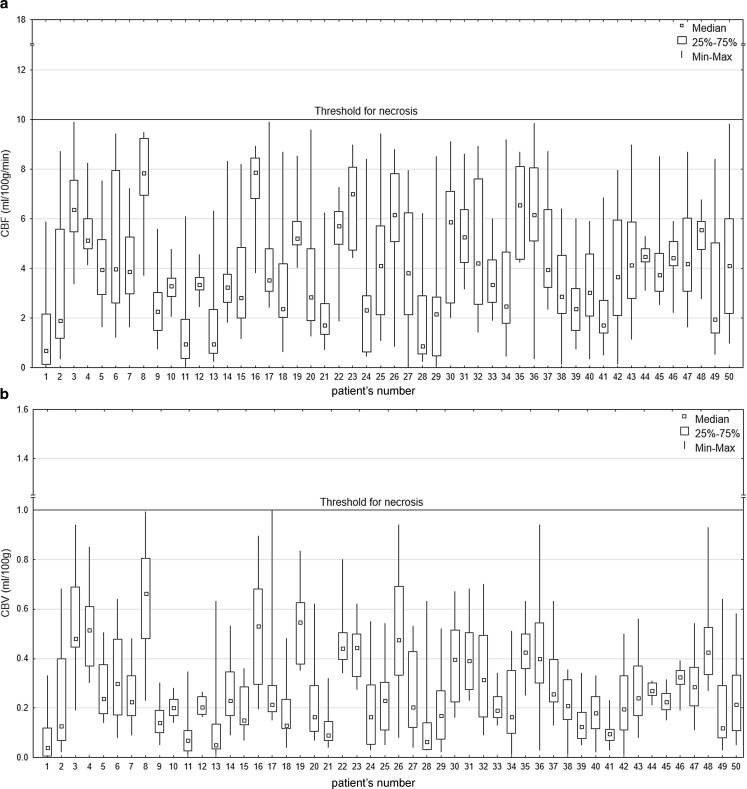
Material and methods: Whole brain CTP was performed in patients in the intensive care unit diagnosed with BD and CTA was derived from CTP datasets. Cerebral blood flow (CBF) and volume (CBV) were calculated in all brain regions. The CTP findings were interpreted as being consistent with a diagnosis of BD (positive) when CBF and CBV in all regions of interest (ROIs) were below 10 ml/100 g/min and 1.0 ml/100 g, respectively. The CTA findings were interpreted using a 4-point grading system.
Results: A total of 50 patients were included in the study. The CTP results revealed CBF from 0.00 to 9.98 ml/100 g/min (mean, 1.98 ± 1.68 ml/100 g/min) and CBV from 0.00 to 0.99 ml/100 g (mean, 0.14 ± 0.12 ml/100 g) and were thus interpreted as positive in all 50 patients. In contrast, the CTA results suggested 7 negative cases, providing a sensitivity of 86%. The difference between the CTP and CTA sensitivity results for the diagnosis of BD was statistically significant (p = 0.006).
Conclusion: Whole brain CTP may potentially be a feasible and highly sensitive test for diagnosing BD: therefore, performing CTP in combination with CTA in cases when CTA results are negative for BD could increase the sensitivity of CTA.
Keywords: Brain death; Four-dimensional computed tomography; Multidetector computed tomography; Perfusion imaging.
Conflict of interest statement
M. Sawicki, J. Sołek-Pastuszka, K. Chamier-Ciemińska, A. Walecka, J. Walecki and R. Bohatyrewicz declare that they have no competing interests.
Figures
Comment in
-
Neuroimaging of Intracranial Perfusion and the Clinical Diagnosis of Brain Death: Setting the Gold Standard in Humans.Clin Neuroradiol. 2019 Sep;29(3):575-577. doi: 10.1007/s00062-019-00806-z. Epub 2019 Jul 9. Clin Neuroradiol. 2019. PMID: 31289876 No abstract available.
References
-
- Wijdicks EF, Varelas PN, Gronseth GS, Greer DM, American Academy of Neurology Evidence-based guideline update: determining brain death in adults: report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2010;74(23):1911–1918. doi: 10.1212/WNL.0b013e3181e242a8. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
