

Directional local field potentials: A tool to optimize deep brain stimulation
- PMID: 29150884
- PMCID: PMC5768242
- DOI: 10.1002/mds.27215
Directional local field potentials: A tool to optimize deep brain stimulation
Abstract
Background: Although recently introduced directional DBS leads provide control of the stimulation field, programing is time-consuming.
Objectives: Here, we validate local field potentials recorded from directional contacts as a predictor of the most efficient contacts for stimulation in patients with PD.
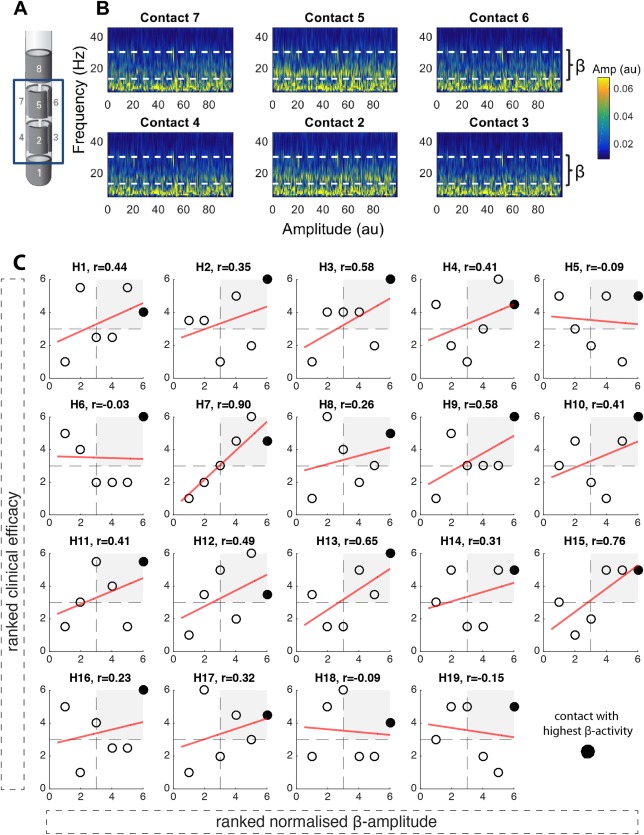
Methods: Intraoperative local field potentials were recorded from directional contacts in the STN of 12 patients and beta activity compared with the results of the clinical contact review performed after 4 to 7 months.
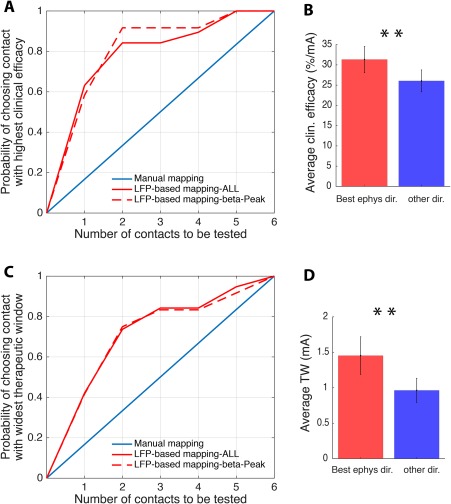
Results: Normalized beta activity was positively correlated with the contact's clinical efficacy. The two contacts with the highest beta activity included the most efficient stimulation contact in up to 92% and that with the widest therapeutic window in 74% of cases.
Conclusion: Local field potentials predict the most efficient stimulation contacts and may provide a useful tool to expedite the selection of the optimal contact for directional DBS. © 2017 The Authors. Movement Disorders published by Wiley Periodicals, Inc. on behalf of International Parkinson and Movement Disorder Society.
Keywords: DBS programming; Parkinson's disease; deep brain stimulation; directional leads; local field potentials.
© 2017 The Authors. Movement Disorders published by Wiley Periodicals, Inc. on behalf of International Parkinson and Movement Disorder Society.
Figures
Comment in
-
Next generation programming.Mov Disord. 2018 Feb;33(2):186. doi: 10.1002/mds.27322. Epub 2018 Jan 25. Mov Disord. 2018. PMID: 29369418 No abstract available.
References
-
- Pollo C, Kaelin‐Lang A, Oertel MF, et al. Directional deep brain stimulation: an intraoperative double‐blind pilot study. Brain 2014;137:2015‐2026. - PubMed
-
- Timmermann L, Jain R, Chen L, et al. Multiple‐source current steering in subthalamic nucleus deep brain stimulation for Parkinson's disease (the VANTAGE study): a non‐randomised, prospective, multicentre, open‐label study. Lancet Neurol 2015;14:693‐701. - PubMed
-
- Contarino MF, Bour LJ, Verhagen R, et al. Directional steering: a novel approach to deep brain stimulation. Neurology 2014;83:1163‐1169. - PubMed
-
- Reker P, Dembek TA, Becker J, et al. Directional deep brain stimulation: a case of avoiding dysarthria with bipolar directional current steering. Parkinsonism Relat Disord 2016;31:156‐158. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
