

Isolated Adrenocorticotropin Deficiency due to Nivolumab-induced Hypophysitis in a Patient with Advanced Lung Adenocarcinoma: A Case Report and Literature Review
- PMID: 29151505
- PMCID: PMC5849549
- DOI: 10.2169/internalmedicine.9074-17
Isolated Adrenocorticotropin Deficiency due to Nivolumab-induced Hypophysitis in a Patient with Advanced Lung Adenocarcinoma: A Case Report and Literature Review
Abstract
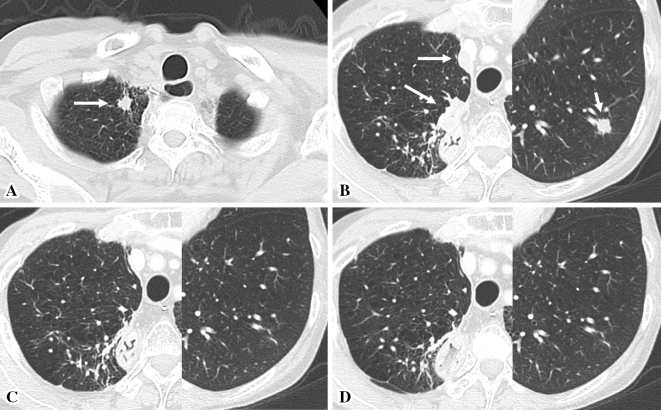
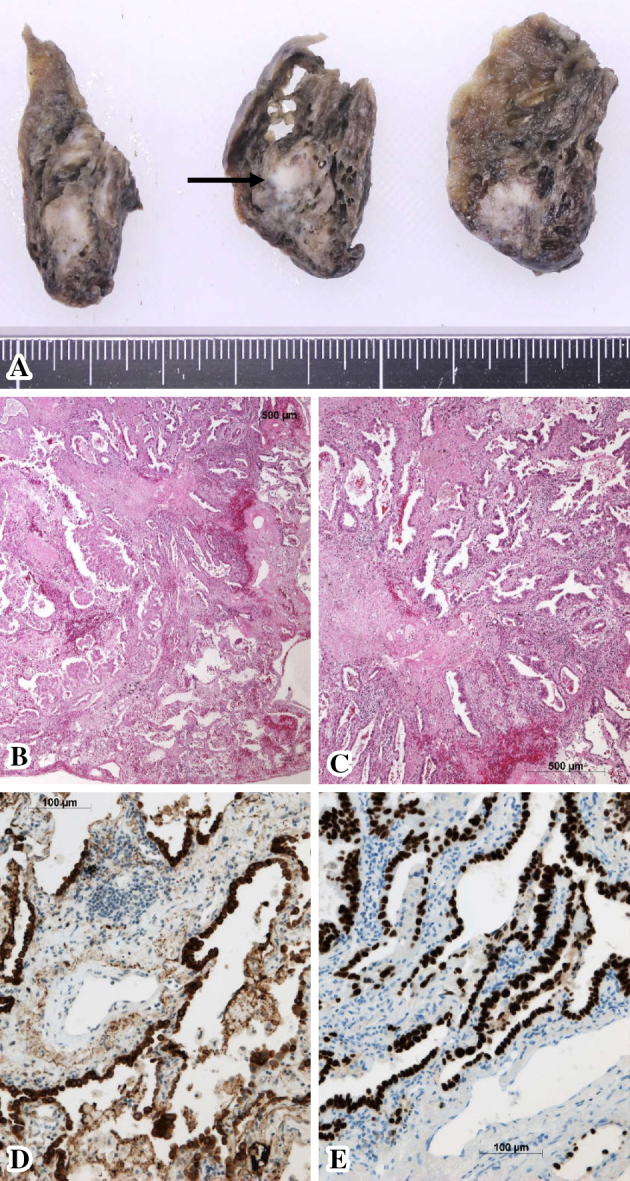
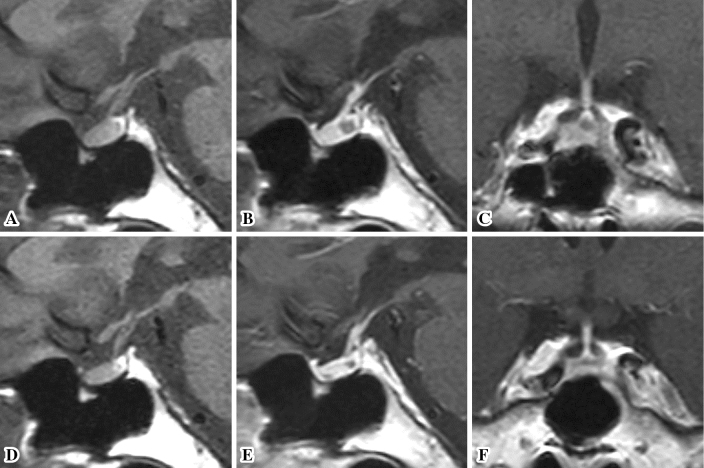
A 63-year-old Japanese woman with advanced lung adenocarcinoma developed isolated adrenocorticotropin deficiency caused by immune checkpoint inhibitor (ICI)-related hypophysitis following 8 months of nivolumab therapy. Prompt corticosteroid replacement therapy effectively relieved her secondary adrenal insufficiency symptoms and allowed her to pursue nivolumab therapy, which had been effective for the control of lung adenocarcinoma. Human leukocyte antigen (HLA) typing revealed the presence of the DRB1*04:05-DQA1*03:03-DQB1*04:01 haplotype, which is associated with susceptibility to autoimmune polyglandular syndrome with pituitary disorder in the Japanese population. This case suggests that genetic factors, such as HLA, contribute to the development of endocrinopathies induced by ICIs.
Keywords: human leukocyte antigen; hydrocortisone; hypophysitis; lung adenocarcinoma; nivolumab.
Figures
Similar articles
-
Isolated adrenocorticotropic hormone deficiency associated with sintilimab therapy in a patient with advanced lung adenocarcinoma: a case report and literature review.BMC Endocr Disord. 2022 Sep 24;22(1):239. doi: 10.1186/s12902-022-01151-y. BMC Endocr Disord. 2022. PMID: 36153581 Free PMC article. Review.
-
Isolated adrenocorticotropic hormone deficiency and thyroiditis associated with nivolumab therapy in a patient with advanced lung adenocarcinoma: a case report and review of the literature.J Med Case Rep. 2019 Mar 26;13(1):88. doi: 10.1186/s13256-019-2002-2. J Med Case Rep. 2019. PMID: 30909965 Free PMC article. Review.
-
Isolated Adrenocorticotropic Hormone Deficiency Caused by Nivolumab in a Patient with Metastatic Lung Cancer.Intern Med. 2017 Sep 15;56(18):2463-2469. doi: 10.2169/internalmedicine.8548-16. Epub 2017 Aug 21. Intern Med. 2017. PMID: 28824067 Free PMC article.
-
Nivolumab-induced Hypophysitis, Secondary Adrenal Insufficiency and Destructive Thyroiditis in a Patient with Lung Adenocarcinoma.Intern Med. 2019 Mar 1;58(5):693-697. doi: 10.2169/internalmedicine.1268-18. Epub 2018 Nov 19. Intern Med. 2019. PMID: 30449786 Free PMC article.
-
Nivolumab-induced hypophysitis causing secondary adrenal insufficiency after transient ACTH elevation.Endocr J. 2019 Oct 28;66(10):937-941. doi: 10.1507/endocrj.EJ19-0076. Epub 2019 Jun 19. Endocr J. 2019. PMID: 31217401
Cited by
-
Nivolumab-induced hypophysitis leading to hypopituitarism and secondary empty sella syndrome in a patient with non-small cell lung cancer.BMJ Case Rep. 2019 Mar 7;12(3):e228135. doi: 10.1136/bcr-2018-228135. BMJ Case Rep. 2019. PMID: 30850565 Free PMC article.
-
A case of small-cell lung cancer with adrenocorticotropic hormone deficiency induced by nivolumab.Onco Targets Ther. 2019 Mar 25;12:2181-2186. doi: 10.2147/OTT.S194094. eCollection 2019. Onco Targets Ther. 2019. PMID: 30988622 Free PMC article.
-
Adverse Effects of Immune Checkpoint Inhibitors (Programmed Death-1 Inhibitors and Cytotoxic T-Lymphocyte-Associated Protein-4 Inhibitors): Results of a Retrospective Study.J Clin Med Res. 2019 Apr;11(4):225-236. doi: 10.14740/jocmr3750. Epub 2019 Mar 18. J Clin Med Res. 2019. PMID: 30937112 Free PMC article. Review.
-
Hypopituitarism induced by pembrolizumab plus axitinib in the treatment of metastatic renal cell carcinoma: A case report.Oncol Lett. 2023 Dec 20;27(2):66. doi: 10.3892/ol.2023.14199. eCollection 2024 Feb. Oncol Lett. 2023. PMID: 38192652 Free PMC article.
-
Isolated adrenocorticotropic hormone deficiency associated with sintilimab therapy in a patient with advanced lung adenocarcinoma: a case report and literature review.BMC Endocr Disord. 2022 Sep 24;22(1):239. doi: 10.1186/s12902-022-01151-y. BMC Endocr Disord. 2022. PMID: 36153581 Free PMC article. Review.
References
-
- Andrioli M, Pecori Giraldi F, Cavagnini F. Isolated corticotrophin deficiency. Pituitary 9: 289-295, 2006. - PubMed
-
- Michot JM, Bigenwald C, Champiat S, et al. . Immune-related adverse events with immune checkpoint blockade: a comprehensive review. Eur J Cancer 54: 139-148, 2016. - PubMed
-
- Torino F, Corsello SM, Salvatori R. Endocrinological side-effects of immune checkpoint inhibitors. Curr Opin Oncol 28: 278-287, 2016. - PubMed
-
- Falorni A, Minarelli V, Bartoloni E, Alunno A, Gerli R. Diagnosis and classification of autoimmune hypophysitis. Autoimmun Rev 13: 412-416, 2014. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials