

Multiple guided technologies based on radial probe endobronchial ultrasound for the diagnosis of solitary peripheral pulmonary lesions: a single-center study
- PMID: 29151936
- PMCID: PMC5687166
- DOI: 10.7150/jca.20035
Multiple guided technologies based on radial probe endobronchial ultrasound for the diagnosis of solitary peripheral pulmonary lesions: a single-center study
Abstract
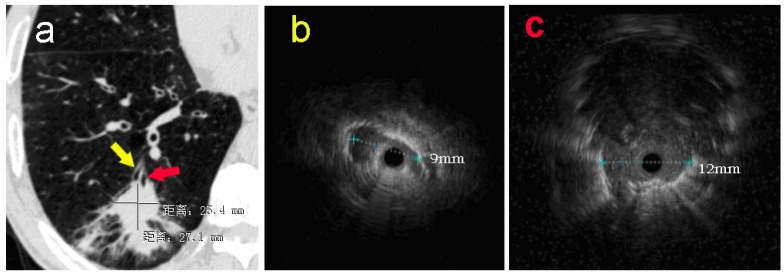
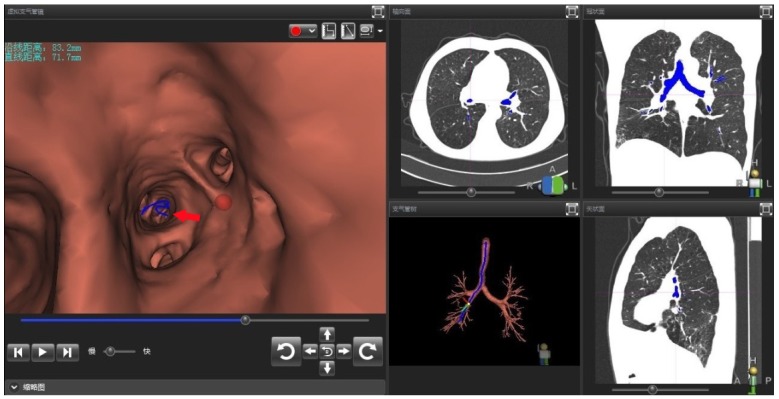
Objective To evaluate the value of multiple guided technologies based on radial probe endobronchial ultrasound (R-EBUS) in the application of the diagnosis of solitary pulmonary peripheral lesions (PPLs). Methods Analysis of diagnostic yield in 4 groups patients with different combined multiple guided technologies based on R-EBUS, 94 patients with 94 solitary PPLs from Mar, 2013 to Nov, 2014 in Changhai Hospital. Results The overall diagnostic yield was 75% (70/94), the diagnostic yield of Group A (R-EBUS) was 62%(16/26), Group B (R-EBUS with guided sheath, EBUS-GS) was 76% (34/45), Group C (EBUS-GS with fluoroscopy) was 82% (9/11), Group D (virtual bronchoscopic navigation guided EBUS-GS with fluoroscopy) was 92% (11/12). The overall histopathological diagnostic yield was 56% (53/94. Better histopathological diagnostic yield was associated with application of multiple guided technologies based on EBUS-GS, lesions located in non-lower lobes, lesion's diameter > 2cm, radial probe within the lesions and lidocaine nebulization combined with intravenous anesthesia. There were no severe complications in all the 94 cases. A ultrasonic radial probe was broken when exploring a lesion located in the apical-posterior segment of left upper lobe. Conclusion Multiple guided technologies based on R-EBUS were safe and effective in the diagnosis of solitary PPLs. In practice, the diagnosis yield improved with the application of forcep biopsies combined with bronchial brushing and washing.
Keywords: EBUS-GS; biopsy; bronchoscope; diagnosis; endobronchial ultrasound; fluoroscopy; peripheral pulmonary lesion; radial probe; virtual bronchial navigation (VBN).
Conflict of interest statement
Competing Interests: The authors have declared that no competing interest exists.
Figures
References
-
- Rivera MP MA, Wahidi MM. Establishing the diagnosis of lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. 3rd ed: CHEST; 2013. - PubMed
-
- Asano F. Recommendation of Combination of Radial Endobronchial Ultrasound With Virtual Bronchoscopic Navigation. Journal of bronchology & interventional pulmonology. 2016;23:187–8. doi:10.1097/LBR.0000000000000301. - PubMed
-
- Asano F. Advanced bronchoscopy for the diagnosis of peripheral pulmonary lesions. Respiratory investigation. 2016;54:224–9. doi:10.1016/j.resinv.2015.11.008. - PubMed
-
- Herth FJ, Ernst A, Becker HD. Endobronchial ultrasound-guided transbronchial lung biopsy in solitary pulmonary nodules and peripheral lesions. The European respiratory journal. 2002;20:972–4. - PubMed
-
- Gex G, Pralong JA, Combescure C, Seijo L, Rochat T, Soccal PM. Diagnostic yield and safety of electromagnetic navigation bronchoscopy for lung nodules: a systematic review and meta-analysis. Respiration; international review of thoracic diseases. 2014;87:165–76. doi:10.1159/000355710. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
