

Robotic transduodenal excision of ampullary tumour
- PMID: 29152477
- PMCID: PMC5673755
- DOI: 10.21037/hbsn.2016.12.04
Robotic transduodenal excision of ampullary tumour
Abstract
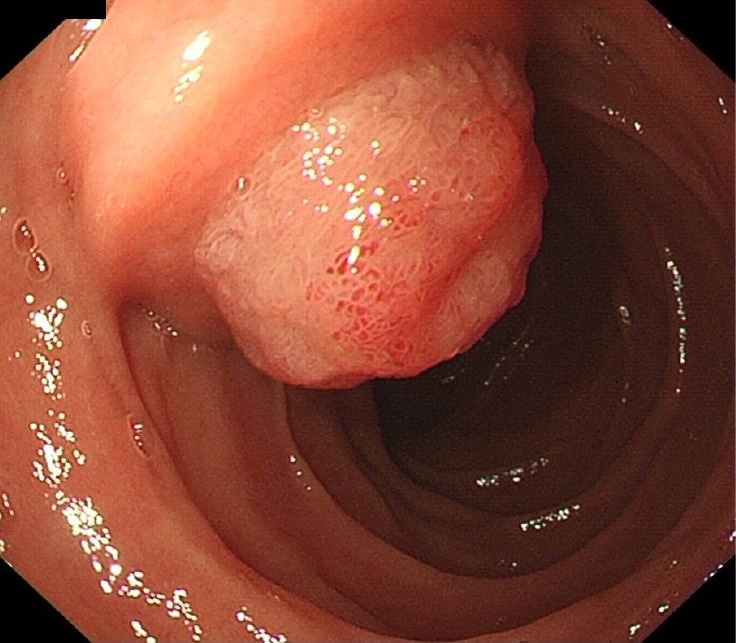
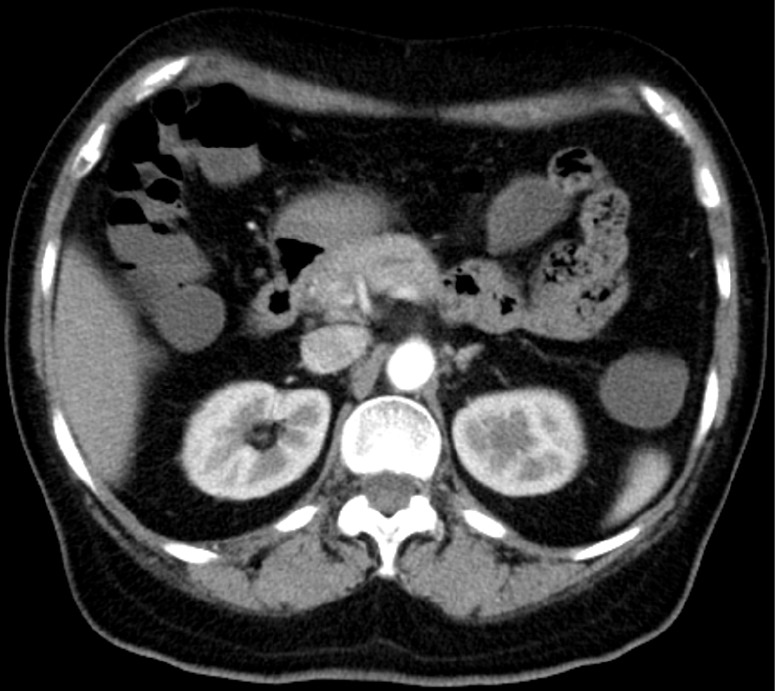
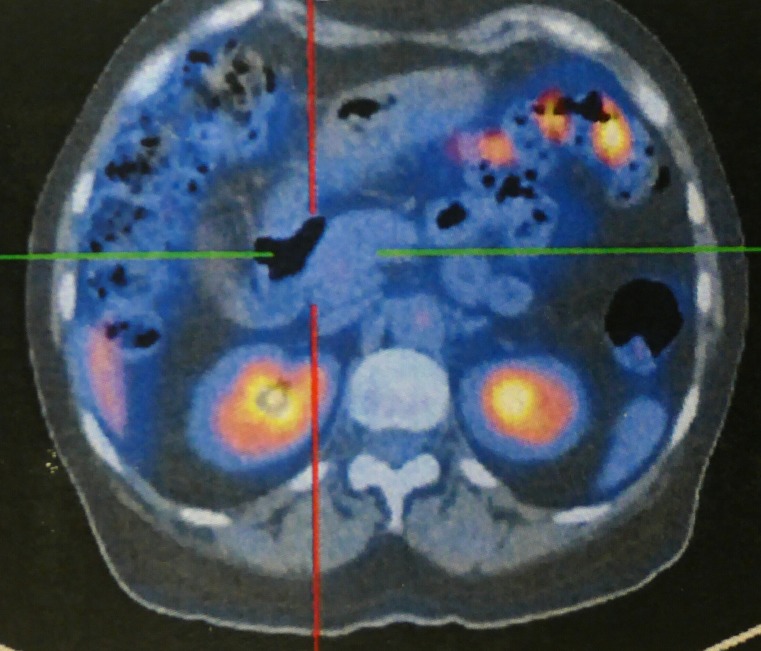
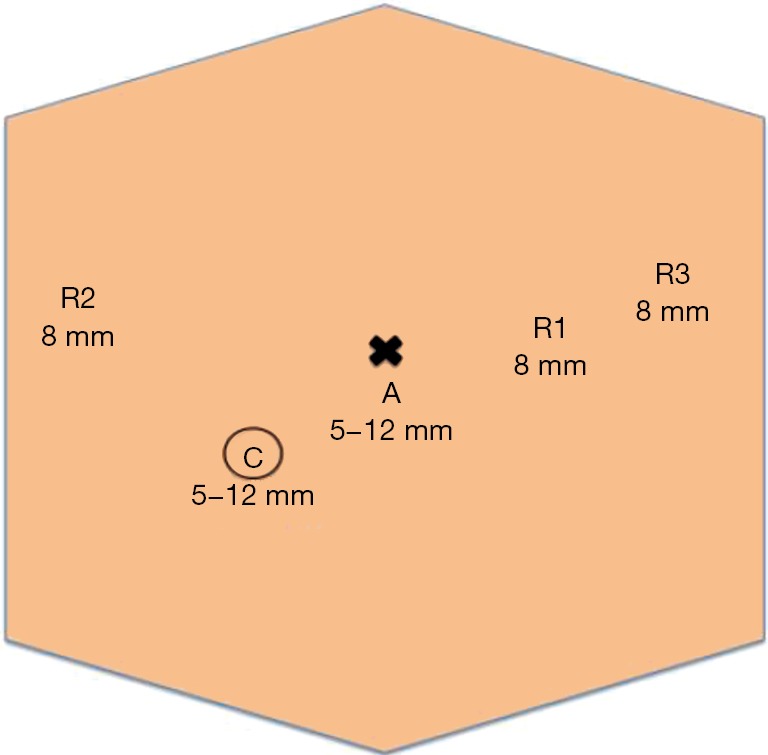
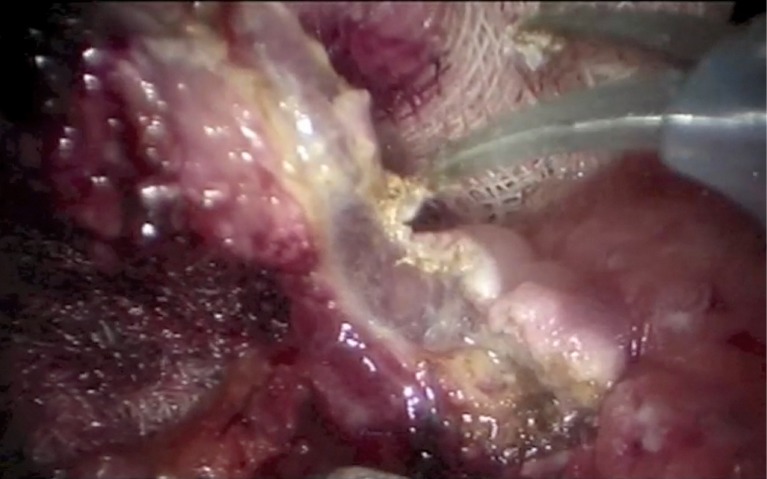
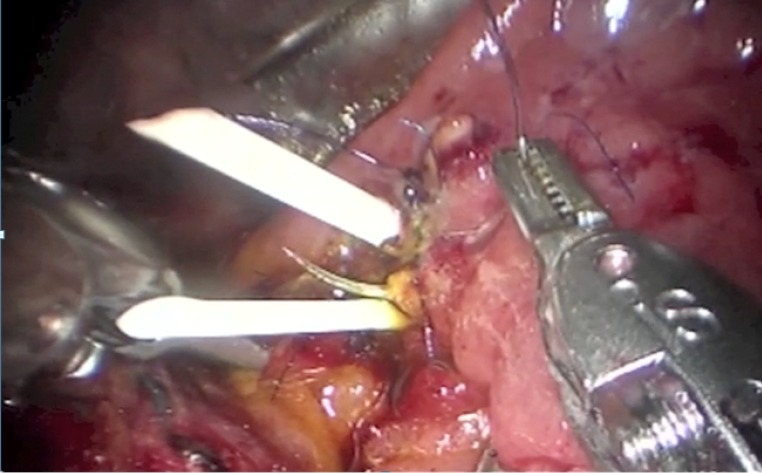
Ampullary tumours are uncommon lesions with potential risk of malignancy. The management is excision by either endoscopic ampullectomy, pancreaticoduodenectomy or transduodenal excision. Endoscopic ampullectomy offers a less invasive approach, whereas pancreaticoduodenectomy allows radical excision of the tumour. They both carry their own limitations. Transduodenal excision of ampullary tumour offers significantly lower risks with low recurrence rate, and can be offered for benign or early grade tumours. Limited cases of laparoscopic transduodenal excision of ampullary tumours were reported in the literature, probably due to the technical difficulties in performing the operation, especially during the reconstruction of the pancreaticobiliary ducts with the laparoscopic approach. In the era with robotic surgical systems, the technical demanding procedures are greatly facilitated. Hence, we are writing to report a case of transduodenal excision of ampullary tumour with the robot assisted laparoscopic approach.
Keywords: Robotic; ampulla; operative technique; transduodenal excision; tumour.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources