

Diabetes, metabolic comorbidities, and risk of hepatocellular carcinoma: Results from two prospective cohort studies
- PMID: 29152763
- PMCID: PMC5906170
- DOI: 10.1002/hep.29660
Diabetes, metabolic comorbidities, and risk of hepatocellular carcinoma: Results from two prospective cohort studies
Abstract
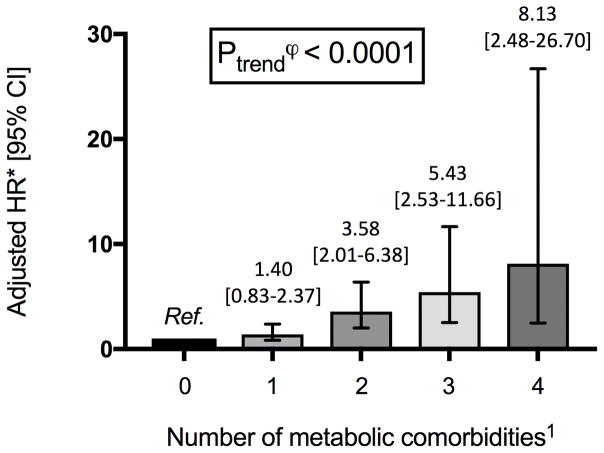
Type 2 diabetes (T2D) is a risk factor for hepatocellular carcinoma (HCC). However, it is unknown whether T2D duration or additional metabolic comorbidities further contribute to HCC risk. From the Nurses' Health Study (NHS), 120,826 women were enrolled in 1980, and from the Health Professionals Follow-up Study (HPFS), 50,284 men were enrolled in 1986 and followed through 2012. Physician-diagnosed T2D was ascertained at baseline and updated biennially. Cox proportional hazards regression models were used to calculate age- and multivariable-adjusted hazard ratios (HRs) and 95% confidence intervals (CIs) for incident HCC. Over 32 years of follow-up (4,488,410 person-years), we documented 112 cases of HCC (69 women, 43 men). T2D was associated with an increased HCC risk (multivariable HR, 4.59; 95% CI, 2.98-7.07), as was an increasing T2D duration (Ptrend < 0.001). Compared to nondiabetics, the multivariable HRs for HCC were 2.96 (95% CI, 1.57-5.60) for 0-<2 years; 6.08 (95% CI, 2.96-12.50) for 2-<10 years; and 7.52 (95% CI, 3.88-14.58) for ≥10 years. Increasing number of metabolic comorbidities (T2D, obesity, hypertension, and dyslipidemia) was associated with increased HCC risk (Ptrend < 0.001); compared to individuals without metabolic comorbidity, those with four metabolic comorbidities had an 8.1-fold increased HCC risk (95% CI, 2.48-26.7). In T2D, neither insulin use nor oral hypoglycemic use was significantly associated with HCC risk (HR, 2.04 [95% CI, 0.69-6.09] and HR, 1.45 [95% CI, 0.69-3.07], respectively).
Conclusion: T2D is independently associated with increased risk for HCC in two prospective cohorts of U.S. men and women. This risk is enhanced with prolonged diabetes duration and with comorbid metabolic conditions, suggesting the importance of insulin resistance in the pathogenesis of HCC. (Hepatology 2018;67:1797-1806).
© 2017 by the American Association for the Study of Liver Diseases.
Conflict of interest statement
The remaining authors have no disclosures and no conflicts of interest to disclose.
Figures
References
-
- Group IDFDA. Update of mortality attributable to diabetes for the IDF Diabetes Atlas: estimates for the year 2011. Diabetes Res Clin Pract. 2013;100:277–9. - PubMed
-
- Geiss LS, Wang J, Cheng YJ, et al. Prevalence and incidence trends for diagnosed diabetes among adults aged 20 to 79 years, United States, 1980–2012. JAMA. 2014;312:1218–26. - PubMed
-
- Calle EE, Rodriguez C, Walker-Thurmond K, et al. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N Engl J Med. 2003;348:1625–38. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
