

Cost-effectiveness Analyses of Antihypertensive Medicines: A Systematic Review
- PMID: 29153114
- PMCID: PMC5836308
- DOI: 10.1016/j.amepre.2017.06.020
Cost-effectiveness Analyses of Antihypertensive Medicines: A Systematic Review
Abstract
Context: Hypertension affects one third of the U.S. adult population. Although cost-effectiveness analyses of antihypertensive medicines have been published, a comprehensive systematic review across medicine classes is not available.
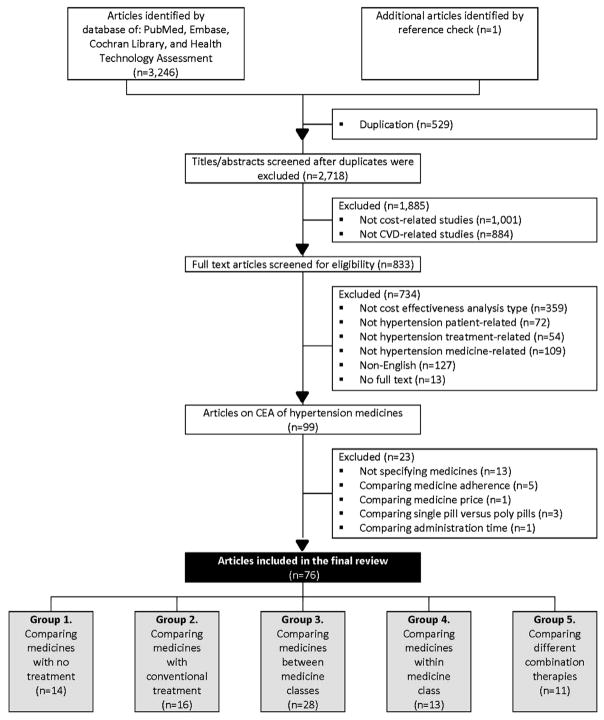
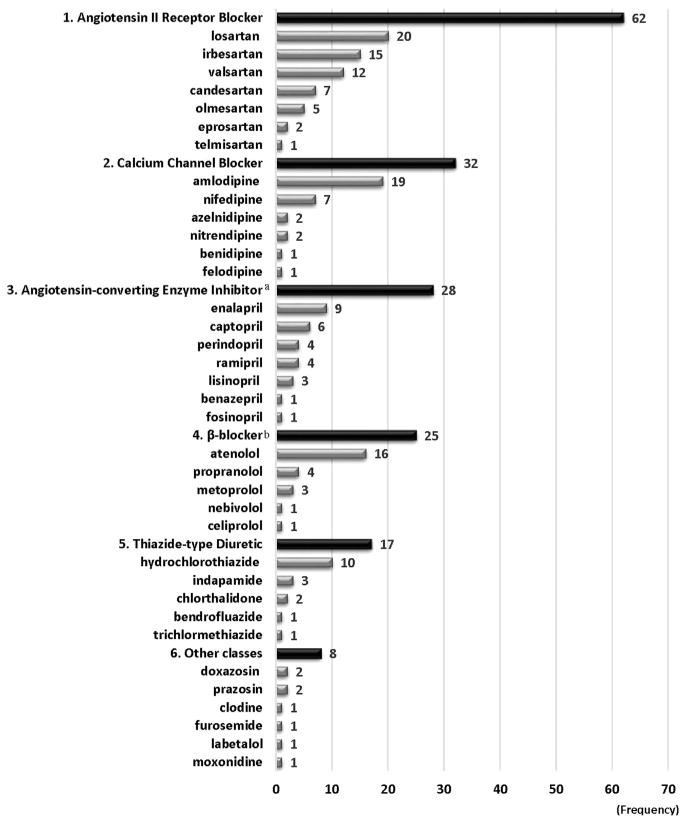
Evidence acquisition: PubMed, Embase, Cochrane Library, and Health Technology Assessment were searched to identify original cost-effectiveness analyses published from 1990 through August 2016. Results were summarized by medicine class: angiotensin-converting enzyme inhibitors (ACEIs), angiotensin receptor blockers (ARBs), calcium channel blockers (CCBs), thiazide-type diuretics, β-blockers, and others. Incremental cost-effectiveness ratios (ICERs) were adjusted to 2015 U.S. dollars.
Evidence synthesis: Among 76 studies reviewed, 14 compared medicines with no treatment, 16 compared medicines with conventional therapy, 29 compared between medicine classes, 13 compared within medicine class, and 11 compared combination therapies. All antihypertensives were cost effective compared with no treatment (ICER/quality-adjusted life year [QALY]=dominant-$19,945). ARBs were more cost effective than CCBs (ICER/QALY=dominant-$13,016) in nine comparisons, whereas CCBs were more cost effective than ARBs (ICER/QALY=dominant) in two comparisons. ARBs were more cost effective than ACEIs (ICER/QALY=dominant-$34,244) and β-blockers (ICER/QALY=$1,498-$18,137) in all eight comparisons.
Conclusions: All antihypertensives were cost effective compared with no treatment. ARBs appeared to be more cost effective than CCBs, ACEIs, and β-blockers. However, these latter findings should be interpreted with caution because these findings are not robust due to the substantial variability across the studies, including study settings and analytic models, changes in the cost of generic medicines, and publication bias.
Published by Elsevier Inc.
Figures
References
-
- CDC. Vital signs: prevalence, treatment, and control of hypertension—United States, 1999–2002 and 2005–2008. MMWR Morb Mortal Wkly Rep. 2011;60(4):103–108. - PubMed
-
- Benjamin EJ, Blaha MJ, Chiuve SE, et al. Heart disease and stroke statistics–2017 update: a report from the American Heart Association. Circulation. 2017;135(10):e146–e603. https://doi.org/10.1161/CIR.0000000000000485. - DOI - PMC - PubMed
-
- Davis K. Expenditures for Hypertension among Adults Age 18 and Older, 2010: Estimates for the U.S. Civilian Noninstitutionalized Population. Statistical Brief #404. Rockville, MD: Agency for Healthcare Research and Quality; Apr, 2013. - PubMed
-
- Neal B, MacMahon S, Chapman N Blood Pressure Lowering Treatment Trialists’ Collaboration. Effects of ACE inhibitors, calcium antagonists, and other blood-pressure-lowering drugs: results of prospectively designed overviews of randomised trials. Blood Pressure Lowering Treatment Trialists’ Collaboration. Lancet. 2000;356(9246):1955–1964. https://doi.org/10.1016/S0140-6736(00)03307-9. - DOI - PubMed
-
- Balu S, Thomas J., 3rd Incremental expenditure of treating hypertension in the United States. Am J Hypertens. 2006;19(8):810–816. https://doi.org/10.1016/j.amjhyper.2005.12.013. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
