

Image-based ex-vivo drug screening for patients with aggressive haematological malignancies: interim results from a single-arm, open-label, pilot study
- PMID: 29153976
- PMCID: PMC5719985
- DOI: 10.1016/S2352-3026(17)30208-9
Image-based ex-vivo drug screening for patients with aggressive haematological malignancies: interim results from a single-arm, open-label, pilot study
Abstract
Background: Patients with refractory or relapsed haematological malignancies have few treatment options and short survival times. Identification of effective therapies with genomic-based precision medicine is hampered by intratumour heterogeneity and incomplete understanding of the contribution of various mutations within specific cancer phenotypes. Ex-vivo drug-response profiling in patient biopsies might aid effective treatment identification; however, proof of its clinical utility is limited.
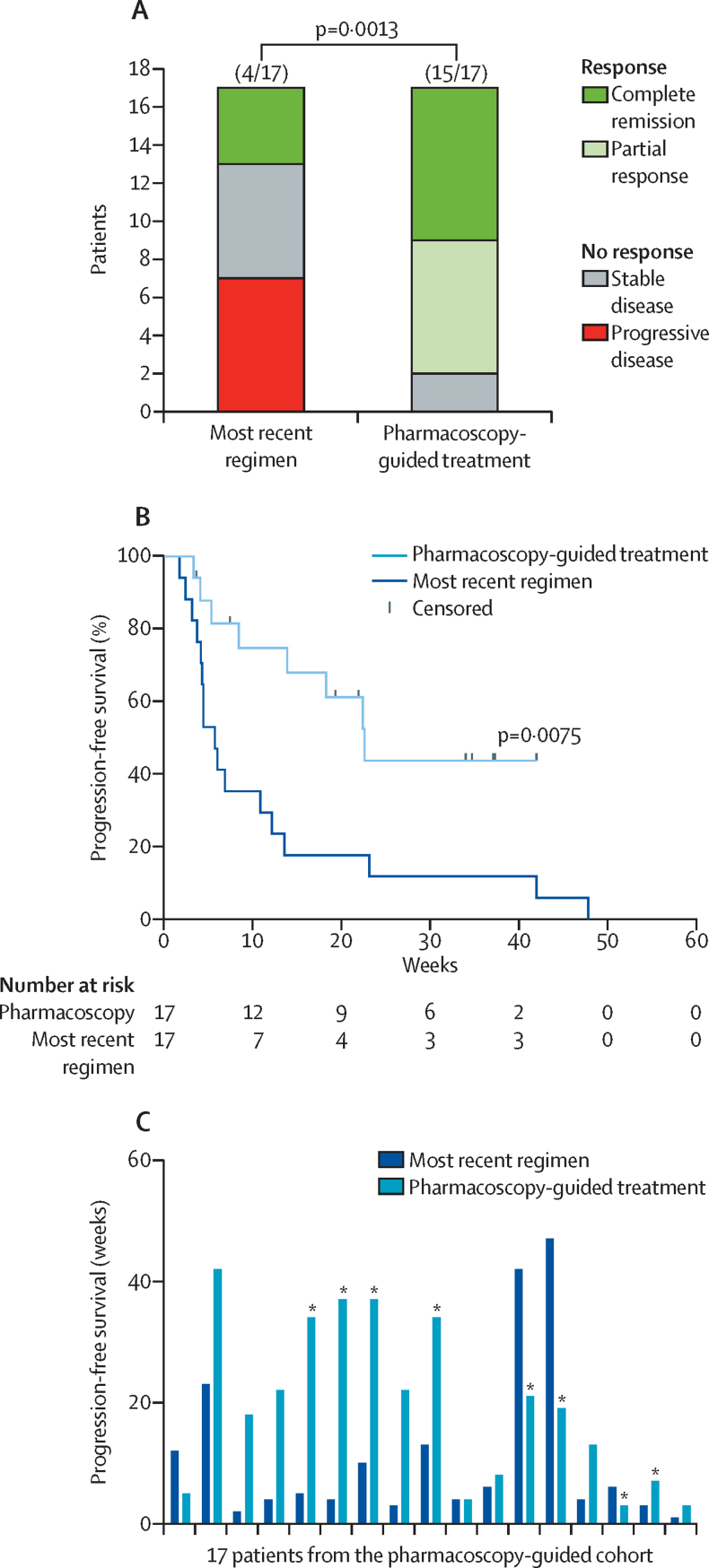
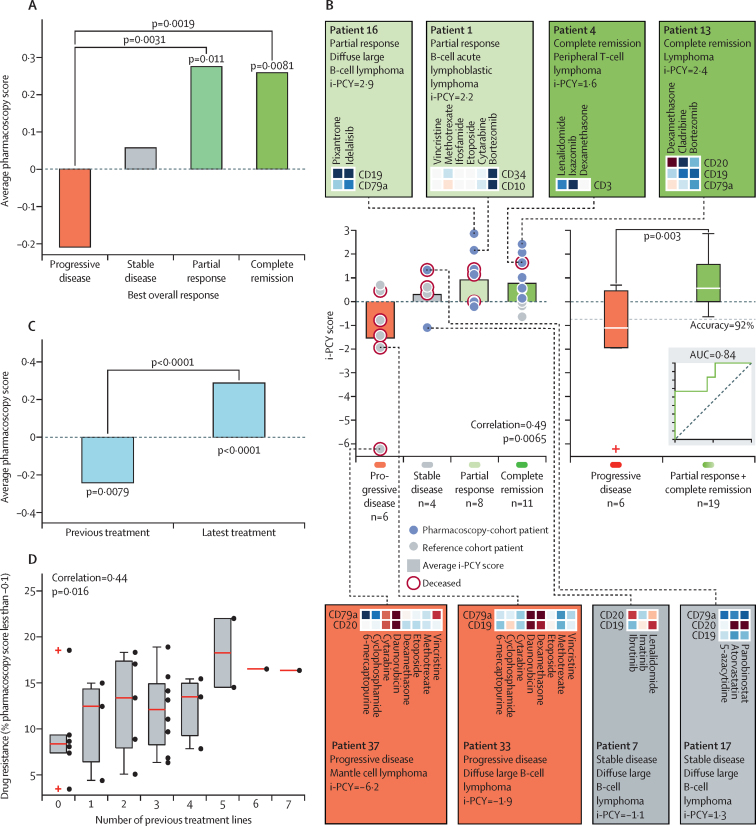
Methods: We investigated the feasibility and clinical impact of multiparametric, single-cell, drug-response profiling in patient biopsies by immunofluorescence, automated microscopy, and image analysis, an approach we call pharmacoscopy. First, the ability of pharmacoscopy to separate responders from non-responders was evaluated retrospectively for a cohort of 20 newly diagnosed and previously untreated patients with acute myeloid leukaemia. Next, 48 patients with aggressive haematological malignancies were prospectively evaluated for pharmacoscopy-guided treatment, of whom 17 could receive the treatment. The primary endpoint was progression-free survival in pharmacoscopy-treated patients, as compared with their own progression-free survival for the most recent regimen on which they had progressive disease. This trial is ongoing and registered with ClinicalTrials.gov, number NCT03096821.
Findings: Pharmacoscopy retrospectively predicted the clinical response of 20 acute myeloid leukaemia patients to initial therapy with 88·1% accuracy. In this interim analysis, 15 (88%) of 17 patients receiving pharmacoscopy-guided treatment had an overall response compared with four (24%) of 17 patients with their most recent regimen (odds ratio 24·38 [95% CI 3·99-125·4], p=0·0013). 12 (71%) of 17 patients had a progression-free survival ratio of 1·3 or higher, and median progression-free survival increased by four times, from 5·7 (95% CI 4·1-12·1) weeks to 22·6 (7·4-34·0) weeks (hazard ratio 3·14 [95% CI 1·37-7·22], p=0·0075).
Interpretation: Routine clinical integration of pharmacoscopy for treatment selection is technically feasible, and led to improved treatment of patients with aggressive refractory haematological malignancies in an initial patient cohort, warranting further investigation.
Funding: Austrian Academy of Sciences; European Research Council; Austrian Science Fund; Austrian Federal Ministry of Science, Research and Economy; National Foundation for Research, Technology and Development; Anniversary Fund of the Austrian National Bank; MPN Research Foundation; European Molecular Biology Organization; and Swiss National Science Foundation.
Copyright © 2017 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures


Comment in
-
A precision medicine approach to haematological malignancies.Lancet Haematol. 2017 Dec;4(12):e567-e568. doi: 10.1016/S2352-3026(17)30213-2. Epub 2017 Nov 15. Lancet Haematol. 2017. PMID: 29153977 No abstract available.
References
-
- Khwaja A, Bjorkholm M, Gale RE. Acute myeloid leukaemia. Nat Rev Dis Primers. 2016;2:16010. - PubMed
-
- Hood L, Friend SH. Predictive, personalized, preventive, participatory (P4) cancer medicine. Nat Rev Clin Oncol. 2011;8:184–187. - PubMed
-
- Von Hoff DD, Stephenson JJ, Jr, Rosen P. Pilot study using molecular profiling of patients' tumors to find potential targets and select treatments for their refractory cancers. J Clin Oncol. 2010;28:4877–4883. - PubMed
-
- Le Tourneau C, Delord JP, Goncalves A. Molecularly targeted therapy based on tumour molecular profiling versus conventional therapy for advanced cancer (SHIVA): a multicentre, open-label, proof-of-concept, randomised, controlled phase 2 trial. Lancet Oncol. 2015;16:1324–1334. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
