

Risk of Upgrading from Prostate Biopsy to Radical Prostatectomy Pathology-Does Saturation Biopsy of Index Lesion during Multiparametric Magnetic Resonance Imaging-Transrectal Ultrasound Fusion Biopsy Help?
- PMID: 29154904
- PMCID: PMC7983157
- DOI: 10.1016/j.juro.2017.10.048
Risk of Upgrading from Prostate Biopsy to Radical Prostatectomy Pathology-Does Saturation Biopsy of Index Lesion during Multiparametric Magnetic Resonance Imaging-Transrectal Ultrasound Fusion Biopsy Help?
Abstract
Purpose: We sought to determine whether saturation of the index lesion during magnetic resonance imaging-transrectal ultrasound fusion guided biopsy would decrease the rate of pathological upgrading from biopsy to radical prostatectomy.
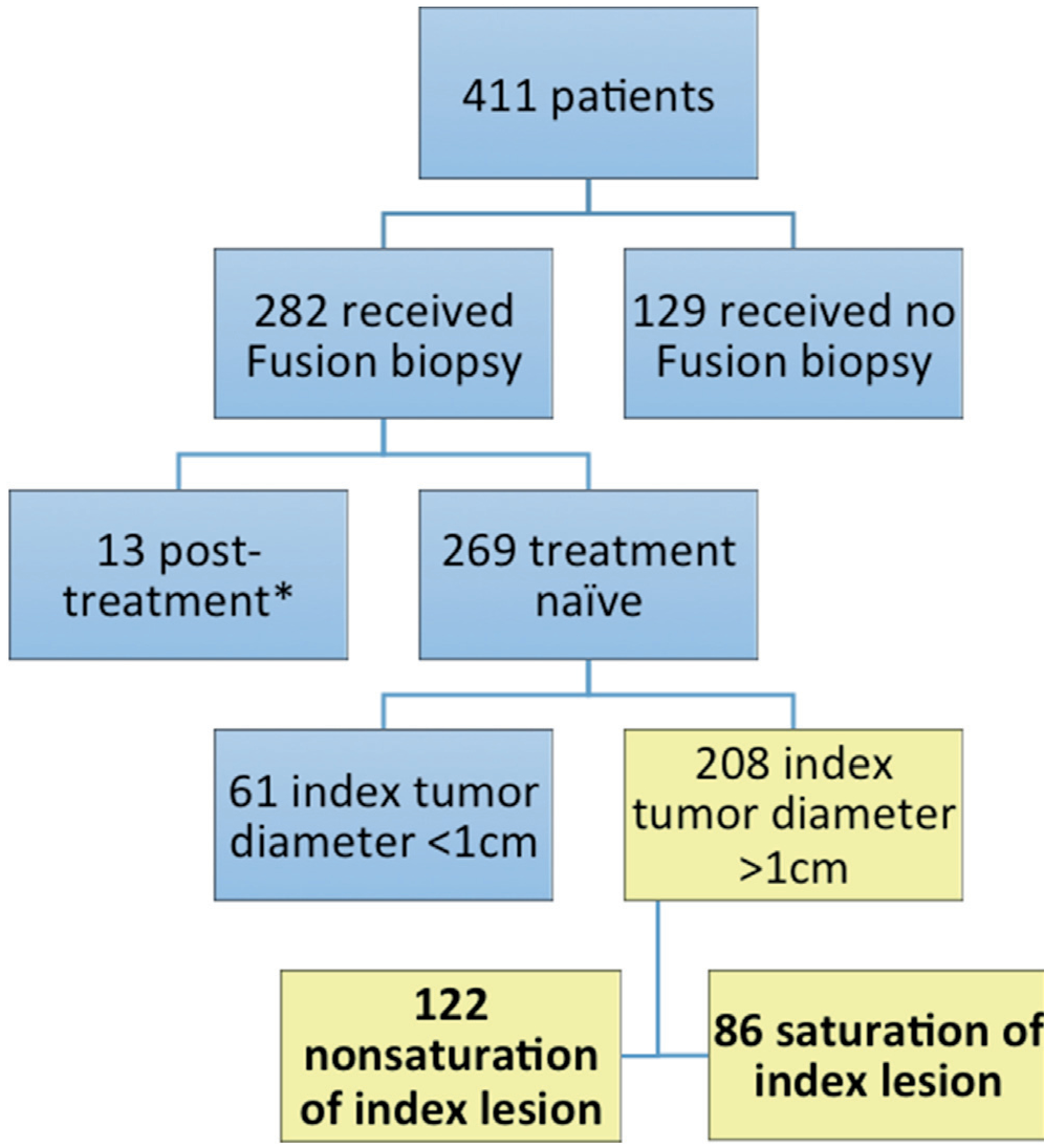
Materials and methods: We analyzed a prospectively maintained, single institution database for patients who underwent fusion and systematic biopsy followed by radical prostatectomy in 2010 to 2016. Index lesion was defined as the lesion with largest diameter on T2-weighted magnetic resonance imaging. In patients with a saturated index lesion transrectal fusion biopsy targets were obtained at 6 mm intervals along the long axis of the index lesion. In patients with a nonsaturated index lesion only 1 target was obtained from the lesion. Gleason 6, 7 and 8-10 were defined as low, intermediate and high risk, respectively.
Results: Included in the study were 208 consecutive patients, including 86 with a saturated and 122 with a nonsaturated lesion. Median patient age was 62.0 years (IQR 10.0) and median prostate specific antigen was 7.1 ng/ml (IQR 8.0). The median number of biopsy cores per index lesion was higher in the saturated lesion group (4 vs 2, p <0.001). The risk category upgrade rate from systematic only, fusion only, and combined fusion and systematic biopsy results to prostatectomy was 40.9%, 23.6% and 13.8%, respectively. The risk category upgrade from combined fusion and systematic biopsy results was lower in the saturated than in the nonsaturated lesion group (7% vs 18%, p = 0.021). There was no difference in the upgrade rate based on systematic biopsy between the 2 groups. However, fusion biopsy results were significantly less upgraded in the saturated lesion group (Gleason upgrade 20.9% vs 36.9%, p = 0.014 and risk category upgrade 14% vs 30.3%, p = 0.006).
Conclusions: Our results demonstrate that saturation of the index lesion significantly decreases the risk of upgrading on radical prostatectomy by minimizing the impact of tumor heterogeneity.
Keywords: image-guided biopsy; neoplasm grading; pathology; prostatic neoplasms; risk; surgical.
Copyright © 2018 American Urological Association Education and Research, Inc. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Editorial Comment.J Urol. 2018 Apr;199(4):981-982. doi: 10.1016/j.juro.2017.10.069. Epub 2018 Jan 20. J Urol. 2018. PMID: 29360445 No abstract available.
References
-
- Kvale R, Moller B, Wahlqvist R et al.: Concordance between Gleason scores of needle biopsies and radical prostatectomy specimens: a population-based study. BJU Int 2009; 103: 1647. - PubMed
-
- Fernandes ET, Sundaram CP, Long R et al.: Biopsy Gleason score: how does it correlate with the final pathological diagnosis in prostate cancer? Br J Urol 1997; 79: 615. - PubMed
-
- Borboroglu PG, Comer SW, Riffenburgh RH et al.: Extensive repeat transrectal ultrasound guided prostate biopsy in patients with previous benign sextant biopsies. J Urol 2000; 163: 158. - PubMed
-
- Jiang X, Zhu S, Feng G et al.: Is an initial saturation prostate biopsy scheme better than an extended scheme for detection of prostate cancer? A systematic review and meta-analysis. Eur Urol 2013; 63: 1031. - PubMed
-
- Kahl P, Wolf S, Adam A et al.: Saturation biopsy improves preoperative Gleason scoring of prostate cancer. Pathol Res Pract 2009; 205: 259. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
