

Ambulatory anterior cervical discectomy and fusion is associated with a higher risk of revision surgery and perioperative complications: an analysis of a large nationwide database
- PMID: 29155340
- PMCID: PMC6291305
- DOI: 10.1016/j.spinee.2017.11.012
Ambulatory anterior cervical discectomy and fusion is associated with a higher risk of revision surgery and perioperative complications: an analysis of a large nationwide database
Abstract
Background context: With the changing landscape of health care, outpatient spine surgery is being more commonly performed to reduce cost and to improve efficiency. Anterior cervical discectomy and fusion (ACDF) is one of the most common spine surgeries performed and demand is expected to increase with an aging population.
Purpose: The objective of this study was to determine the nationwide trends and relative complication rates associated with outpatient ACDF.
Study design/setting: This is a large-scale retrospective case control study.
Patient sample: The patient sample included Humana-insured patients who underwent one- to two-level ACDF as either outpatients or inpatients from 2011 to 2016 OUTCOME MEASURES: The outcome measures included incidence and the adjusted odds ratio (OR) of postoperative medical and surgical complications within 1 year of the index surgery.
Materials and methods: A retrospective review was performed of the PearlDiver Humana insurance records database to identify patients undergoing one- to two-level ACDF (Current Procedural Terminology [CPT]-22551 and International Classification of Diseases [ICD]-9-816.2) as either outpatients or inpatients from 2011 to 2016. The incidence of perioperative medical and surgical complications was determined by querying for relevant ICD and CPT codes. Multivariate logistic regression adjusting for age, gender, and Charlson Comorbidity Index was used to calculate ORs of complications among outpatients relative to inpatients undergoing ACDF.
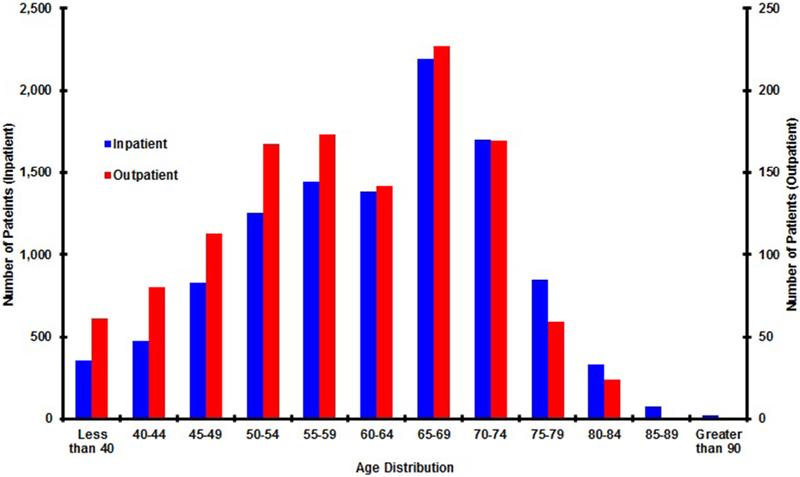
Results: Cohorts of 1,215 patients who underwent outpatient ACDF and 10,964 patients who underwent inpatient ACDF were identified. The median age was in the 65-69 age group for both cohorts. The annual relative incidence of outpatient ACDF increased from 0.11 in 2011 to 0.22 in 2016 (R2=0.82, p=.04). Adjusting for age, gender, and comorbidities, patients undergoing outpatient ACDF were more likely to undergo revision surgery for posterior fusion at both 6 months (OR 1.58, confidence interval [CI] 1.27-1.96, p<.001) and 1 year (OR 1.79, CI 1.51-2.13, p<.001) postoperatively. Outpatient ACDF was also associated with a higher likelihood of revision anterior fusion at 1 year postoperatively (OR 1.46, CI 1.26-1.70, p<.001). Among medical complications, postoperative acute renal failure was more frequently associated with outpatient ACDF than inpatient ACDF (OR 1.25, CI 1.06-1.49, p=.010). Adjusted rates of all other queried surgical and medical complications were comparable.
Conclusions: Outpatient ACDF is increasing in frequency nationwide over the past several years. Nationwide data demonstrate a greater risk of perioperative surgical complications, including revision anterior and posterior fusion, as well as a higher risk of postoperative acute renal failure. Candidates for outpatient ACDF should be counseled and carefully selected to reduce these risks.
Keywords: Ambulatory; Anterior cervical discectomy fusion; Complications; Outpatient; Outpatient spine surgery; Reoperation; Revision surgery.
Published by Elsevier Inc.
Figures
References
-
- McClelland S, Oren JH, Protopsaltis TS, Passias PG. Outpatient anterior cervical discectomy and fusion: a meta-analysis. J Clin Neurosci 2016;34:166–8. - PubMed
-
- Stieber JR, Brown K, Donald GD, Cohen JD. Anterior cervical decompression and fusion with plate fixation as an outpatient procedure. Spine J 2005;5:503–7. - PubMed
-
- Gruskay JA, Fu M, Basques B, Bohl DD, Buerba R, Webb ML, et al. Factors affecting length of stay and complications following elective anterior cervical discectomy and fusion. J Spinal Disord Tech 2014;29:1. - PubMed
-
- Mohandas A, Summa C, Worthington WB, Lerner J, Foley KT, Bohinski RJ, et al. Best practices for outpatient anterior cervical surgery: results from a Delphi panel. Spine 2017;42:E648–59. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
