

Economic and survival burden of dysphagia among inpatients in the United States
- PMID: 29155982
- PMCID: PMC6454833
- DOI: 10.1093/dote/dox131
Economic and survival burden of dysphagia among inpatients in the United States
Abstract
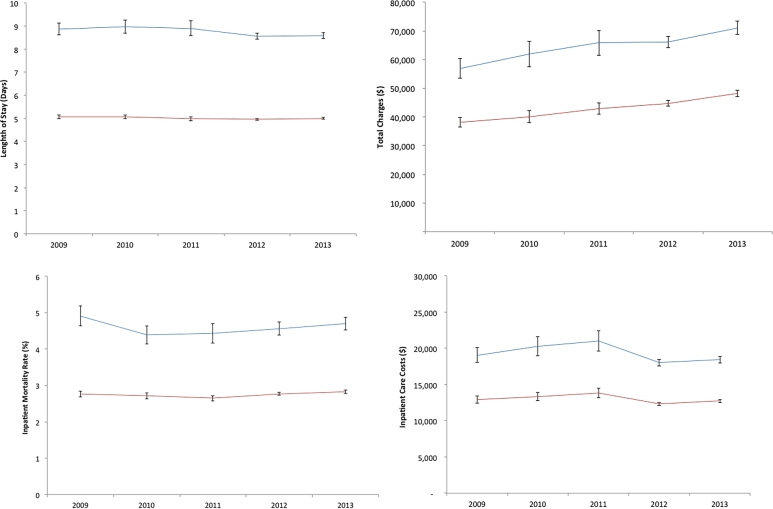
The inpatient burden of dysphagia has primarily been evaluated in patients with stroke. It is unclear whether dysphagia, irrespective of cause, is associated with worse clinical outcomes and higher costs compared to inpatients with similar demographic, hospital, and clinical characteristics without dysphagia. The aim of this study is to assess how a dysphagia diagnosis affects length of hospital stay (LOS), costs, discharge disposition, and in-hospital mortality among adult US inpatients. Annual and overall dysphagia prevalence, LOS, hospital charges, inpatient care costs, discharge disposition, and in-hospital mortality were measured using the AHRQ Healthcare Cost and Utilization Project (HCUP) National Inpatient Sample (2009-2013). Patients aged 45 years or older with ≤180 days of stay in hospital with and without dysphagia were included. Multivariable survey regression methods with propensity weighting were used to assess associations between dysphagia and different outcomes. Overall, 2.7 of 88 million (3.0%) adult US inpatients had a dysphagia diagnosis (50.2% male, 72.4% white, 74.6% age 65-90 years) and prevalence increased from 408,035 (2.5% of admissions) in 2009 to 656,655 (3.3%) in 2013. After inverse probability of treatment weighting adjustment, mean hospital LOS in patients with dysphagia was 8.8 days (95% CI 8.66-8.90) compared to 5.0 days (95% CI 4.97-5.05) in the non-dysphagia group (P < 0.001). Total inpatient costs were a mean $6,243 higher among those with dysphagia diagnoses ($19,244 vs. 13,001, P < 0.001). Patients with dysphagia were 33.2% more likely to be transferred to post-acute care facility (71.9% vs. 38.7%, P < 0.001) with an adjusted OR of 2.8 (95% CI 2.73-2.81, P < 0.001). Compared to non-cases, adult patients with dysphagia were 1.7 times more likely to die in the hospital (95% CI 1.67-1.74). Dysphagia affects 3.0% of all adult US inpatients (aged 45-90 years) and is associated with a significantly longer hospital length of stay, higher inpatient costs, a higher likelihood of discharge to post-acute care facility, and inpatient mortality when compared to those with similar patient, hospital size, and clinical characteristics without dysphagia. Dysphagia has a substantial health and cost burden on the US healthcare system.
Keywords: costs; dysphagia; hospitalization; inpatient; mortality.
© The Authors 2017. Published by Oxford University Press on behalf of International Society for Diseases of the Esophagus. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Cook I J, Kahrilas P J. AGA technical review on management of oropharyngeal dysphagia. Gastroenterology 1999; 116: 455–78. - PubMed
-
- Lindgren S, Janzon L. Prevalence of swallowing complaints and clinical findings among 50-79-year-old men and women in an urban population. Dysphagia 1991; 6: 187–92. - PubMed
-
- Barczi S R, Sullivan P A, Robbins J. How should dysphagia care of older adults differ? Establishing optimal practice patterns. Semin Speech Lang 2000; 21: 347–61. - PubMed
-
- Siebens H, Trupe E, Siebens A et al. Correlates and consequences of eating dependency in institutionalized elderly. J Am Geriatr Soc 1986; 34: 192–8. - PubMed
-
- Bhattacharyya N. The prevalence of dysphagia among adults in the United States. Otolaryngol Head Neck Surg 2014; 151: 765–9. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
