

Immune Activation and Benefit From Avelumab in EBV-Positive Gastric Cancer
- PMID: 29155997
- PMCID: PMC6658862
- DOI: 10.1093/jnci/djx213
Immune Activation and Benefit From Avelumab in EBV-Positive Gastric Cancer
Abstract
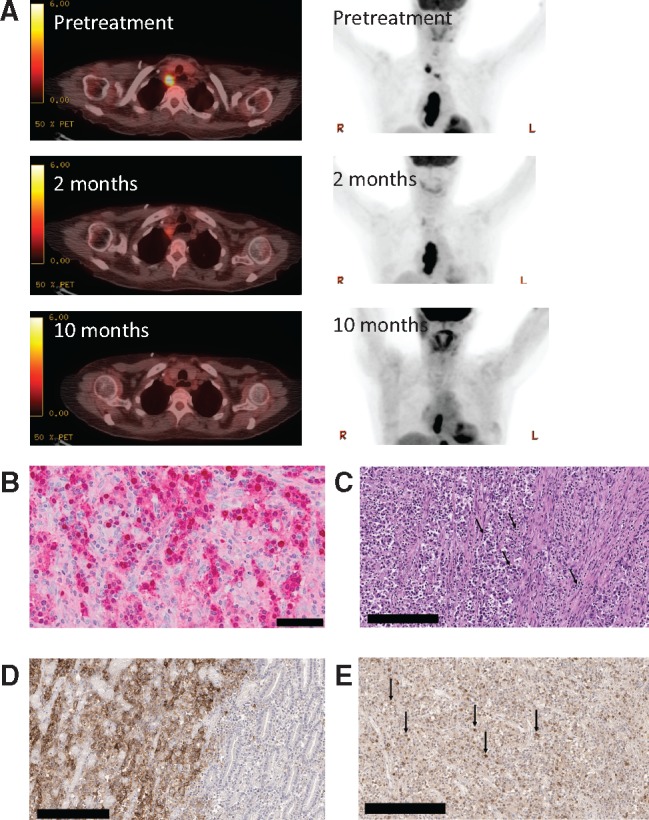
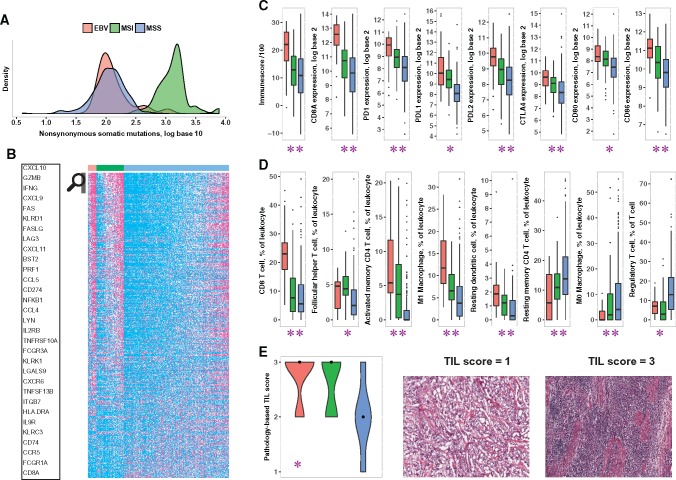
Response to immune checkpoint therapy can be associated with a high mutation burden, but other mechanisms are also likely to be important. We identified a patient with metastatic gastric cancer with meaningful clinical benefit from treatment with the anti-programmed death-ligand 1 (PD-L1) antibody avelumab. This tumor showed no evidence of high mutation burden or mismatch repair defect but was strongly positive for presence of Epstein-Barr virus (EBV) encoded RNA. Analysis of The Cancer Genome Atlas gastric cancer data (25 EBV+, 80 microsatellite-instable [MSI], 310 microsatellite-stable [MSS]) showed that EBV-positive tumors were MSS. Two-sided Wilcoxon rank-sum tests showed that: 1) EBV-positive tumors had low mutation burden (median = 2.07 vs 3.13 in log10 scale, P < 10-12) but stronger evidence of immune infiltration (median ImmuneScore 2212 vs 1295, P < 10-4; log2 fold-change of CD8A = 1.85, P < 10-6) compared with MSI tumors, and 2) EBV-positive tumors had higher expression of immune checkpoint pathway (PD-1, CTLA-4 pathway) genes in RNA-seq data (log2 fold-changes: PD-1 = 1.85, PD-L1 = 1.93, PD-L2 = 1.50, CTLA-4 = 1.31, CD80 = 0.89, CD86 = 1.31, P < 10-4 each), and higher lymphocytic infiltration by histology (median tumor-infiltrating lymphocyte score = 3 vs 2, P < .001) compared with MSS tumors. These data suggest that EBV-positive low-mutation burden gastric cancers are a subset of MSS gastric cancers that may respond to immune checkpoint therapy.
Figures
References
-
- Muro K, Chung HC, Shankaran V et al. , Pembrolizumab for patients with PD-l1-positive advanced gastric cancer (KEYNOTE-012): A multicentre, open-label, phase 1b trial. Lancet Oncol. 2016;176:717–726. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
