

The PREVENT study to evaluate the effectiveness and acceptability of a community-based intervention to prevent childhood tuberculosis in Lesotho: study protocol for a cluster randomized controlled trial
- PMID: 29157275
- PMCID: PMC5697438
- DOI: 10.1186/s13063-017-2184-0
The PREVENT study to evaluate the effectiveness and acceptability of a community-based intervention to prevent childhood tuberculosis in Lesotho: study protocol for a cluster randomized controlled trial
Abstract
Background: Effective, evidence-based interventions to prevent childhood tuberculosis (TB) in high TB/HIV-burden, resource-limited settings are urgently needed. There is limited implementation of evidence-based contact management strategies, including isoniazid preventive therapy (IPT), for child contacts of TB cases in Lesotho.
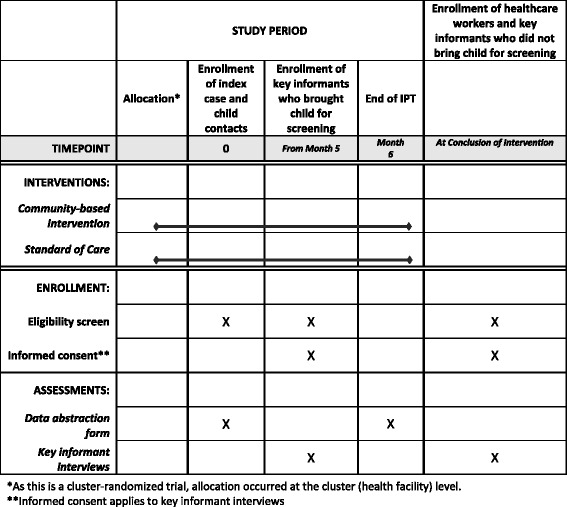
Methods/design: This mixed-methods implementation science study utilizes a two-arm cluster-randomized trial design with randomization at the health facility level. The study aims to evaluate the effectiveness and acceptability of a combination community-based intervention (CBI) versus standard of care (SOC) for the management of child TB contacts. The study includes three phases: (I) exploratory phase; (II) intervention implementation and testing phase; (III) post-intervention explanatory phase. Healthcare provider interviews to inform intervention refinement (phase I) were completed in December 2015. In phase II, 10 health facilities were randomized to deliver the CBI or SOC, with stratification by facility type (i.e., hospital vs. health center). CBI holistically addresses the complex provider-related, patient-related, and caregiver-related barriers to prevention of childhood TB through nurse training and mentorship; health education for caregivers and patients by village health workers; adherence support using text messaging and village health workers; and multidisciplinary team meetings, where programmatic data are reviewed and challenges and solutions are discussed. SOC sites follow country guidelines for child TB contact management. Routine TB program data will be abstracted for all adult TB cases newly registered during the study period and their child contacts from TB registers and cards. The anticipated sample size is 1080 child contacts. Primary outcomes are yield (number) of child contacts, including children < 5 years of age and HIV-positive children < 15 years of age; IPT initiation; and IPT completion. Secondary outcomes include HIV testing; yield of active prevalent TB among child contacts; and acceptability and utilization of CBI components. Intervention implementation began in February 2016 and is ongoing. Post-intervention interviews with healthcare providers and caregivers (phase III) commenced in February 2017.
Discussion: The PREVENT study tests the effectiveness and acceptability of a novel combination CBI for child TB contact management in Lesotho. If effective, CBI will have important implications for addressing childhood TB in Lesotho and elsewhere.
Trial registration: ClinicalTrials.gov, NCT02662829 . Registered on 15 January 2016.
Keywords: Child contact management; Cluster-randomized trial; IPT completion; IPT initiation; Iimplementation science; Intervention acceptability; Intervention effectiveness; Mixed-methods; Ttuberculosis prevention.
Conflict of interest statement
Ethics approval and consent to participate
The protocol was reviewed and approved by the Columbia University Medical Center Institutional Review Board (Ref AAAN7358) and the Lesotho National Health Research and Ethics Committee (Ref ID78-2015). Both regulatory entities determined the medical record review as eligible for waiver of individual consent. Caregivers and healthcare providers who participate in the pre-intervention and post-intervention in-depth interviews provide written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Improving child tuberculosis contact identification and screening in Lesotho: Results from a mixed-methods cluster-randomized implementation science study.PLoS One. 2021 May 20;16(5):e0248516. doi: 10.1371/journal.pone.0248516. eCollection 2021. PLoS One. 2021. PMID: 34014956 Free PMC article.
-
Effectiveness of a community-based intervention to prevent childhood TB in Lesotho.Int J Tuberc Lung Dis. 2022 Jul 1;26(7):612-622. doi: 10.5588/ijtld.21.0558. Int J Tuberc Lung Dis. 2022. PMID: 35768915 Clinical Trial.
-
Community intervention for child tuberculosis active contact investigation and management: study protocol for a parallel cluster randomized controlled trial.Trials. 2021 Mar 2;22(1):180. doi: 10.1186/s13063-021-05124-9. Trials. 2021. PMID: 33653385 Free PMC article.
-
Role of mothers in preventing tuberculosis in children: A scoping review.Narra J. 2024 Dec;4(3):e1062. doi: 10.52225/narra.v4i3.1062. Epub 2024 Sep 30. Narra J. 2024. PMID: 39816113 Free PMC article.
-
Child Contact Case Management-A Major Policy-Practice Gap in High-Burden Countries.Pathogens. 2021 Dec 21;11(1):1. doi: 10.3390/pathogens11010001. Pathogens. 2021. PMID: 35055949 Free PMC article. Review.
Cited by
-
One size does not fit all: preventing tuberculosis among child contacts.BMJ Glob Health. 2019 Dec 29;4(6):e001950. doi: 10.1136/bmjgh-2019-001950. eCollection 2019. BMJ Glob Health. 2019. PMID: 31908872 Free PMC article. No abstract available.
-
Improving child tuberculosis contact identification and screening in Lesotho: Results from a mixed-methods cluster-randomized implementation science study.PLoS One. 2021 May 20;16(5):e0248516. doi: 10.1371/journal.pone.0248516. eCollection 2021. PLoS One. 2021. PMID: 34014956 Free PMC article.
-
Provider attitudes about childhood tuberculosis prevention in Lesotho: a qualitative study.BMC Health Serv Res. 2020 May 25;20(1):461. doi: 10.1186/s12913-020-05324-0. BMC Health Serv Res. 2020. PMID: 32450858 Free PMC article.
-
Implementation of an active, clinic-based child tuberculosis contact management strategy in western Kenya.Public Health Action. 2018 Jun 21;8(2):91-94. doi: 10.5588/pha.17.0119. Public Health Action. 2018. PMID: 29946526 Free PMC article.
-
Toward Developing a Standardized Core Set of Outcome Measures in Mobile Health Interventions for Tuberculosis Management: Systematic Review.JMIR Mhealth Uhealth. 2019 Feb 19;7(2):e12385. doi: 10.2196/12385. JMIR Mhealth Uhealth. 2019. PMID: 30777847 Free PMC article.
References
-
- World Health Organization . Global tuberculosis control: WHO report 2016. Geneva: World Health Organization; 2016.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
