

Insulin Sensitivity and Diabetic Kidney Disease in Children and Adolescents With Type 2 Diabetes: An Observational Analysis of Data From the TODAY Clinical Trial
- PMID: 29157731
- PMCID: PMC5744896
- DOI: 10.1053/j.ajkd.2017.07.015
Insulin Sensitivity and Diabetic Kidney Disease in Children and Adolescents With Type 2 Diabetes: An Observational Analysis of Data From the TODAY Clinical Trial
Erratum in
-
Erratum Regarding "Insulin Sensitivity and Diabetic Kidney Disease in Children and Adolescents With Type 2 Diabetes: An Observational Analysis of Data From the TODAY Clinical Trial" (Am J Kidney Dis. 2018;71[1]:65-74).Am J Kidney Dis. 2019 Apr;73(4):580. doi: 10.1053/j.ajkd.2019.02.001. Epub 2019 Feb 14. Am J Kidney Dis. 2019. PMID: 30773238 Free PMC article. No abstract available.
Abstract
Background: Diabetic kidney disease is a major cause of premature mortality in type 2 diabetes mellitus (T2DM). Worsening insulin sensitivity independent of glycemic control may contribute to the development of diabetic kidney disease. We investigated the longitudinal association of insulin sensitivity with hyperfiltration and increased albumin excretion in adolescents with T2DM.
Study design: Observational prospective cohort study.
Setting & participants: 532 TODAY (Treatment Options for Type 2 Diabetes in Adolescents and Youth) participants aged 12 to 17 years with T2DM duration less than 2 years at baseline. The TODAY Study was a multicenter randomized clinical trial that examined the efficacy of 3 treatment regimens (metformin monotherapy, metformin plus rosiglitazone, or metformin plus an intensive lifestyle intervention program) to achieve durable glycemic control.
Predictors: Natural log-transformed estimated insulin sensitivity (reciprocal of fasting insulin), hemoglobin A1c concentration, age, race-ethnicity, treatment group, body mass index, loss of glycemic control, and hypertension.
Outcomes: Hyperfiltration was defined as 99th percentile or higher of estimated glomerular filtration rate (≥140mL/min/1.73m2) when referenced to healthy adolescents (NHANES 1999-2002) and albumin-creatinine ratio ≥ 30μg/mg at 3 consecutive annual visits.
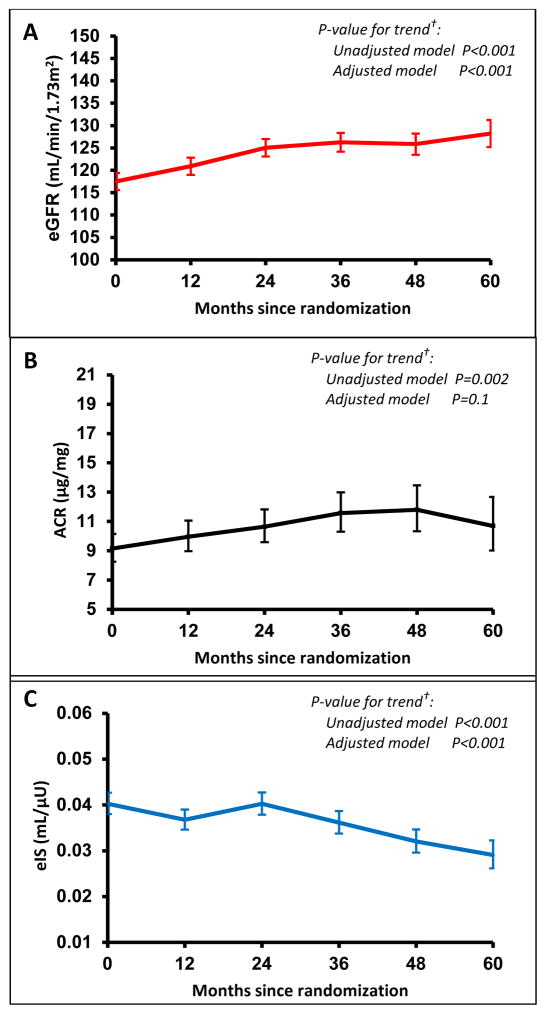
Results: Hyperfiltration was observed in 7.0% of participants at baseline and in 13.3% by 5 years, with a cumulative incidence of 5.0% over 5 years. The prevalence of increased albumin excretion was 6% at baseline and 18% by 5 years, with a cumulative incidence of 13.4%. There was an 8% increase in risk for hyperfiltration per 10% lower estimated insulin sensitivity in unadjusted and adjusted models (P=0.01). Increased albumin excretion was associated with hemoglobin A1c concentration, but not estimated insulin sensitivity.
Limitations: Longer follow-up is needed to capture the transition from hyperfiltration to rapid glomerular filtration rate decline in youth-onset T2DM.
Conclusions: Lower estimated insulin sensitivity was associated with risk for hyperfiltration over time, whereas increased albumin excretion was associated with hyperglycemia in youth-onset T2DM.
Keywords: Type 2 diabetes mellitus (T2DM); adolescents; albumin-creatinine ratio (ACR); children; creatinine; cystatin C; diabetic kidney disease (DKD); disease progression; estimated glomerular filtration rate (eGFR); hyperfiltration; increased albumin excretion; insulin sensitivity; kidney function; youth-onset T2DM.
Copyright © 2017 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Collins AJ, Foley RN, Herzog C, et al. US Renal Data System 2010 Annual Data Report. American journal of kidney diseases: the official journal of the National Kidney Foundation. 2011;57(1 Suppl 1):A8e1–526. - PubMed
-
- Eppens MC, Craig ME, Cusumano J, et al. Prevalence of diabetes complications in adolescents with type 2 compared with type 1 diabetes. Diabetes Care. 2006;29(6):1300–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- UL1 RR024153/RR/NCRR NIH HHS/United States
- UL1 RR025780/RR/NCRR NIH HHS/United States
- M01 RR000069/RR/NCRR NIH HHS/United States
- M01 RR000036/RR/NCRR NIH HHS/United States
- U01 DK061242/DK/NIDDK NIH HHS/United States
- UL1 RR024992/RR/NCRR NIH HHS/United States
- P30 DK036836/DK/NIDDK NIH HHS/United States
- U01 DK061212/DK/NIDDK NIH HHS/United States
- M01 RR001066/RR/NCRR NIH HHS/United States
- M01 RR014467/RR/NCRR NIH HHS/United States
- U01 DK061230/DK/NIDDK NIH HHS/United States
- M01 RR000043/RR/NCRR NIH HHS/United States
- UL1 RR025758/RR/NCRR NIH HHS/United States
- M01 RR000084/RR/NCRR NIH HHS/United States
- UL1 TR002345/TR/NCATS NIH HHS/United States
- U01 DK061254/DK/NIDDK NIH HHS/United States
- T32 DK063687/DK/NIDDK NIH HHS/United States
- UL1 RR024139/RR/NCRR NIH HHS/United States
- UL1 RR024989/RR/NCRR NIH HHS/United States
- M01 RR000125/RR/NCRR NIH HHS/United States
- U01 DK061239/DK/NIDDK NIH HHS/United States
- UL1 RR024134/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
