

Cell type-specific pharmacological kinase inhibition for cancer chemoprevention
- PMID: 29157977
- PMCID: PMC5844817
- DOI: 10.1016/j.nano.2017.11.004
Cell type-specific pharmacological kinase inhibition for cancer chemoprevention
Abstract
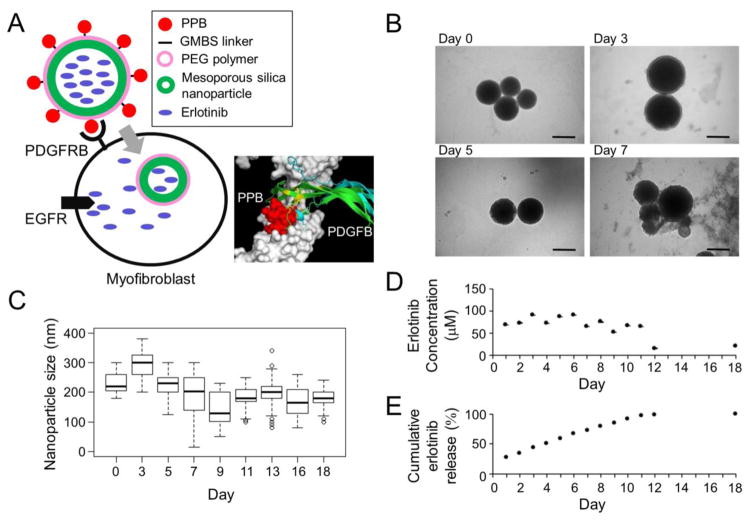
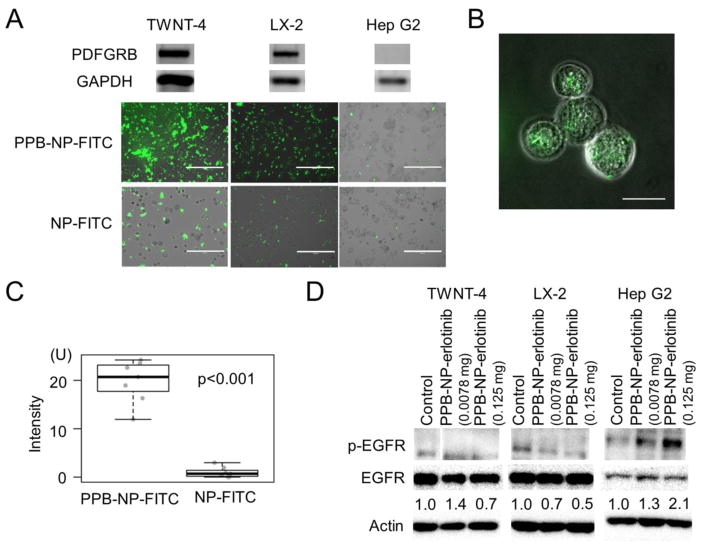
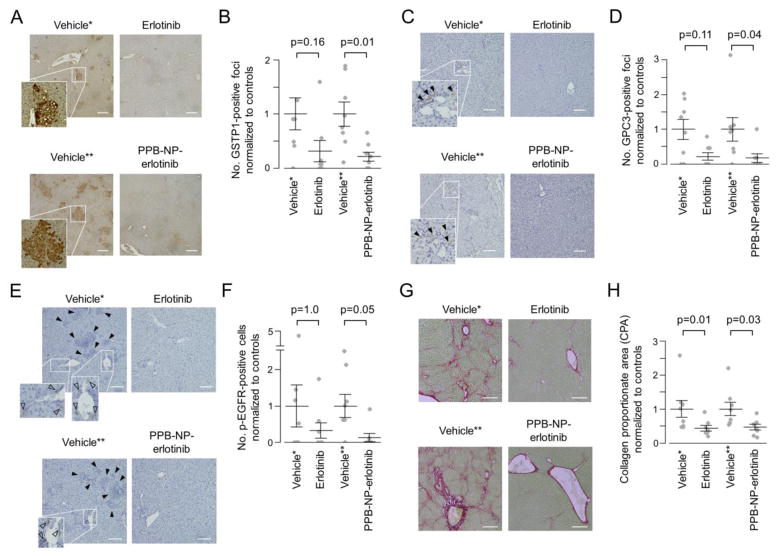
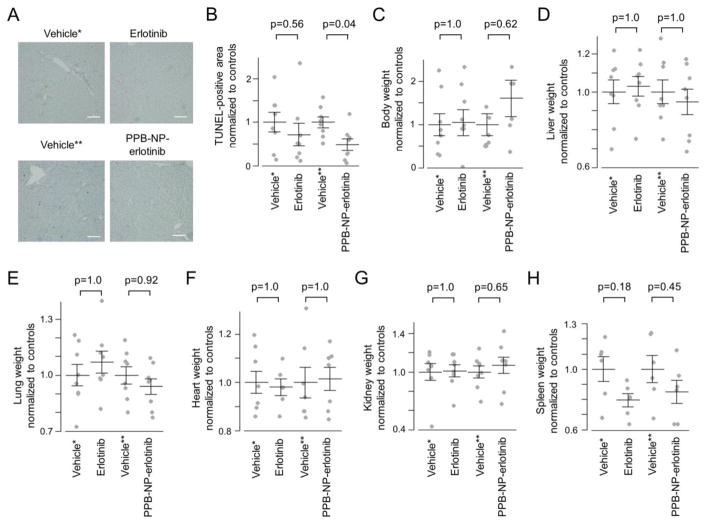
Safety is prerequisite for preventive medicine, but non-toxic agents are generally ineffective as clinical chemoprevention. Here we propose a strategy overcoming this challenge by delivering molecular-targeted agent specifically to the effector cell type to achieve sufficient potency, while circumventing toxicity in the context of cancer chemoprevention. Hepatic myofibroblasts drive progressive fibrosis that results in cirrhosis and liver cancer. In a rat model of cirrhosis-driven liver cancer, a small molecule epidermal growth factor receptor inhibitor, erlotinib, was delivered specifically to myofibroblasts by a versatile nanoparticle-based system, targeting platelet-derived growth factor receptor-beta uniquely expressed on their surface in the liver. With systemic administration of erlotinib, tumor burden was reduced to 31%, which was further improved to 21% by myofibroblast-targeted delivery even with reduced erlotinib dose (7.3-fold reduction with equivalent erlotinib dose) and less hepatocyte damage. These findings demonstrate a strategy, cell type-specific kinase inhibition, for more effective and safer precision cancer chemoprevention.
Keywords: Cancer chemoprevention; Epidermal growth factor; Kinase inhibitor; Liver cancer; Nanoparticle.
Copyright © 2017 Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors have declared that no conflict of interest exists.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
