

Human papillomavirus types from infection to cancer in the anus, according to sex and HIV status: a systematic review and meta-analysis
- PMID: 29158102
- PMCID: PMC5805865
- DOI: 10.1016/S1473-3099(17)30653-9
Human papillomavirus types from infection to cancer in the anus, according to sex and HIV status: a systematic review and meta-analysis
Abstract
Background: Data on carcinogenicity of human papillomavirus (HPV) types in the anus are needed to inform anal cancer prevention through vaccination and screening. This is particularly the case for people infected with HIV, who are at an increased risk of anal cancer.
Methods: We did a systematic review of studies published from January, 1986, to July, 2017, in MEDLINE, Embase, and the Cochrane Library on anal HPV infection, without any language restrictions. Eligible studies reported type-specific HPV prevalence by strata of cytopathological or histopathological anal diagnosis, sex, and HIV status. Data requests were made to authors when necessary. We did a meta-analysis of type-specific HPV prevalence across the full spectrum of anal diagnoses, from normal cytology to anal cancer. We assessed the main outcome of type-specific HPV prevalence ratios [PR], calculated across strata of anal diagnoses, gender, or HIV status, by use of generalised linear models.
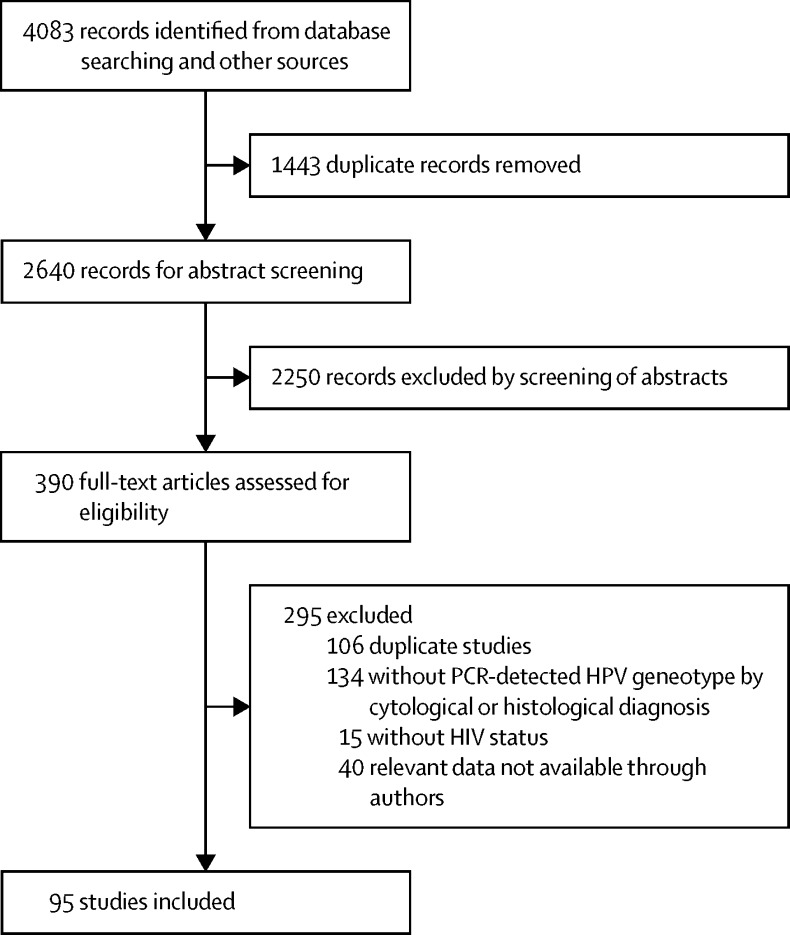
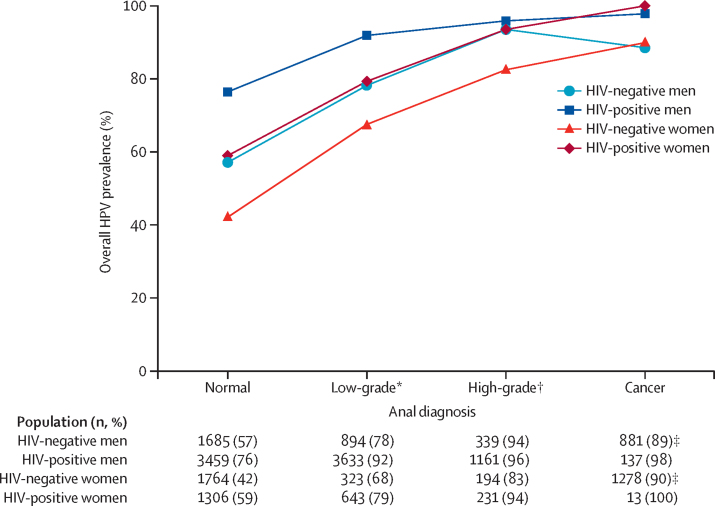
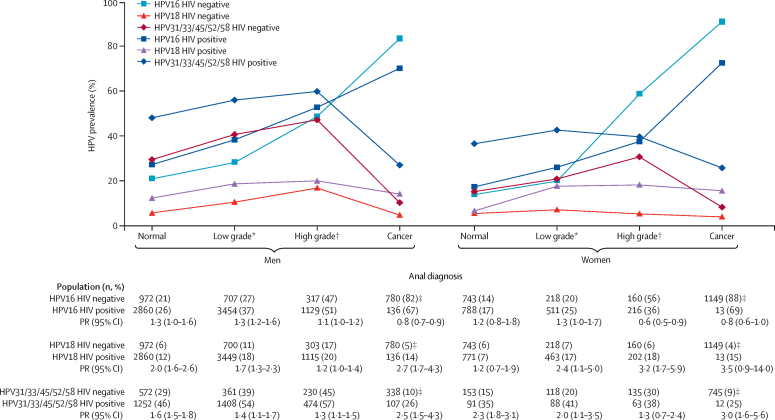
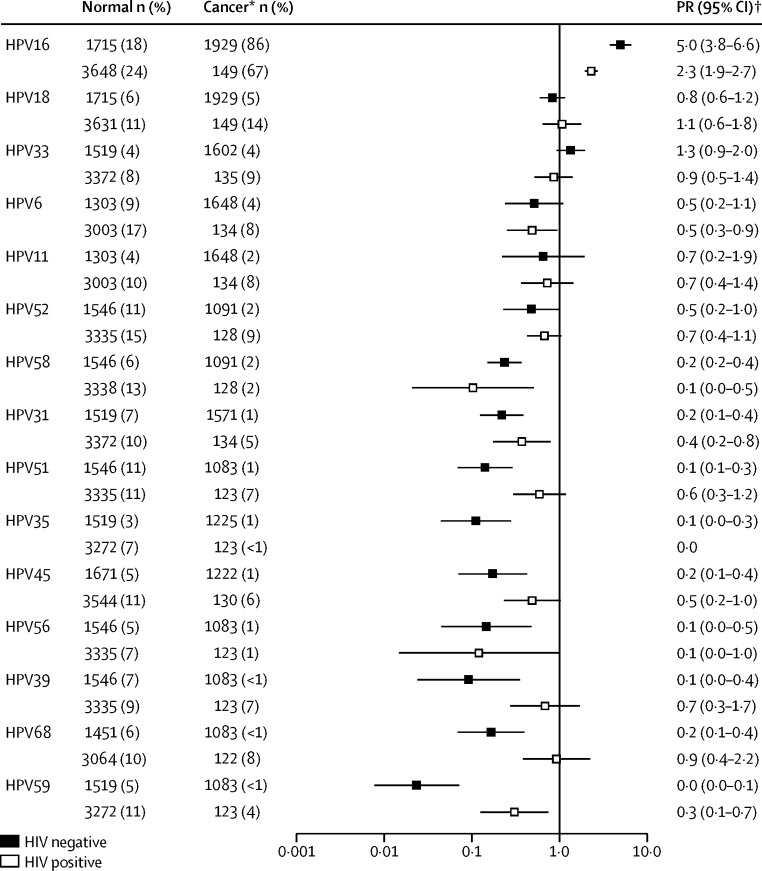
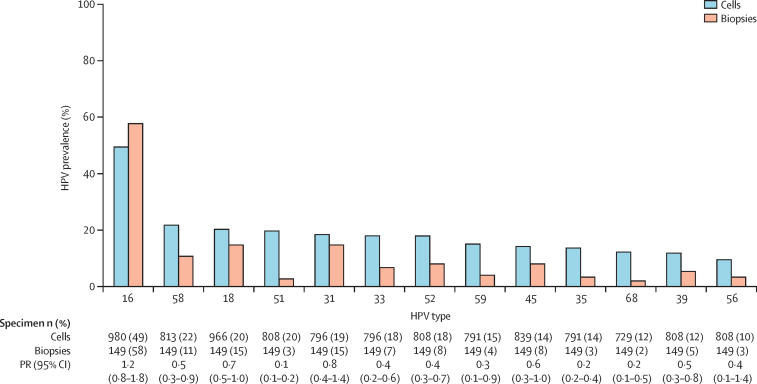
Findings: 95 studies were identified from the search, published between 1992-2017, from which 18 646 individuals fulfilled the criteria for inclusion in the analyses: 8534 people with normal cytology, 5730 with low-grade lesions, 2024 with high-grade lesions, and 2358 with anal cancer. HPV prevalence varied in normal cytology from 42% in HIV-negative women to 76% in HIV-positive men and, for each diagnosis, was higher in individuals who were HIV positive than those who were HIV negative. HPV16 positivity increased with diagnosis severity, being the only HPV type accounting for more HPV infection in anal cancer than normal cytology, both in individuals who were HIV negative (PR 5·0, 95% CI 3·8-6·6, p<0·0001) and those who were HIV positive (2·3, 1·9-2·7, p<0·0001). HPV16 positivity increased even between high-grade lesions and anal cancer, whereas other high-risk HPV types accounted for high proportions of low-grade or high-grade lesions but their prevalence decreased in anal cancer. However, HPV16 was less frequent in HIV-positive than HIV-negative anal cancer, both in men (PR 0·8, 95% CI 0·7-0·9, p<0·0001) and women (0·8, 0·6-1·0, p=0·063), and in HIV-positive versus HIV-negative high-grade lesions in women (0·6, 0·5-0·9, p=0·0077). Type-specific attribution of the non-HPV16 fraction of HIV-positive anal cancer is hindered by a high prevalence of multiple HPV infections.
Interpretation: HPV16 is by far the most carcinogenic HPV type in the anus, with enrichment of HPV16 even from high-grade lesions to anal cancer, both in individuals who are HIV negative and those who are HIV positive. Nevertheless, the fraction of anal cancer attributable to HPV16 is smaller in the HIV-positive population.
Funding: International Agency for Research on Cancer.
Copyright © The Author(s). Published by Elsevier Ltd. This is an Open Access article published under the CC BY-NC-ND 3.0 IGO license which permits users to download and share the article for non-commercial purposes, so long as the article is reproduced in the whole without changes, and provided the original source is properly cited. This article shall not be used or reproduced in association with the promotion of commercial products, services or any entity. There should be no suggestion that IARC endorses any specific organisation, products or services. The use of the IARC logo is not permitted. This notice should be preserved along with the article's original URL.
Figures
Comment in
-
The importance of HPV16 in anal cancer prevention.Lancet Infect Dis. 2018 Feb;18(2):131-132. doi: 10.1016/S1473-3099(17)30683-7. Epub 2017 Nov 17. Lancet Infect Dis. 2018. PMID: 29158103 No abstract available.
References
-
- GLOBOCAN 2012: estimated cancer incidence, mortality and prevalence worldwide in 2012. http://globocan.iarc.fr (accessed May 9, 2017).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
