

Risk Stratification in Arrhythmogenic Right Ventricular Cardiomyopathy
- PMID: 29158215
- PMCID: PMC5777304
- DOI: 10.1161/CIRCULATIONAHA.117.030792
Risk Stratification in Arrhythmogenic Right Ventricular Cardiomyopathy
Abstract
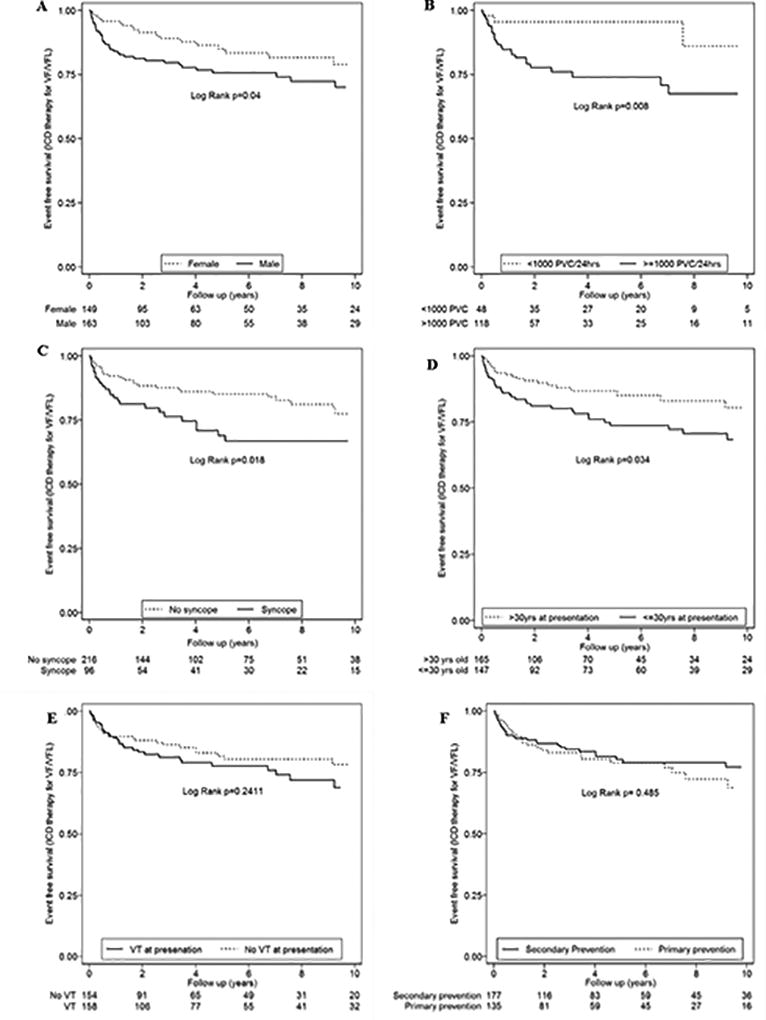
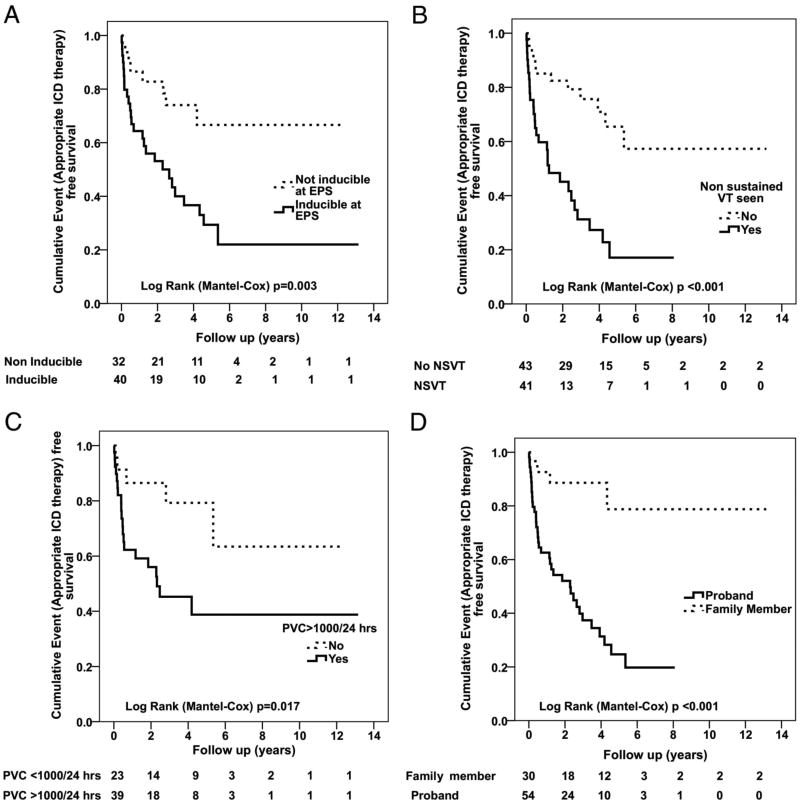
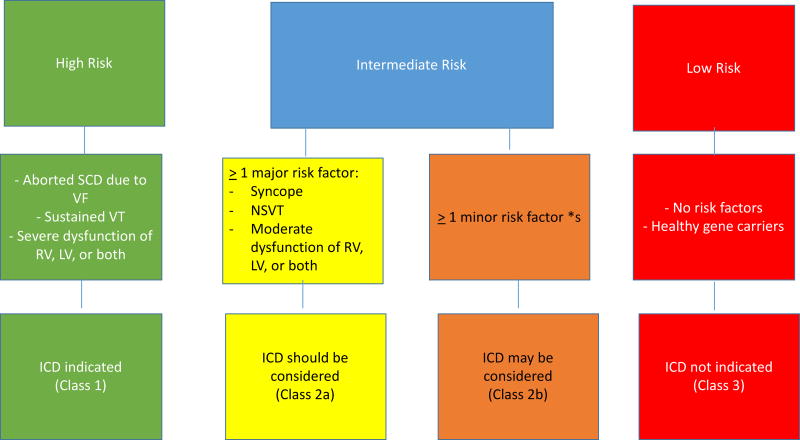
Arrhythmogenic right ventricular cardiomyopathy (ARVC) is an inherited cardiomyopathy characterized by ventricular arrhythmias and an increased risk of sudden cardiac death. Although structural abnormalities of the right ventricle predominate, it is well recognized that left ventricular involvement is common, particularly in advanced disease, and that left-dominant forms occur. The pathological characteristic of ARVC is myocyte loss with fibrofatty replacement. Since the first detailed clinical description of the disorder in 1982, significant advances have been made in understanding this disease. Once the diagnosis of ARVC is established, the single most important clinical decision is whether a particular patient's sudden cardiac death risk is sufficient to justify placement of an implantable cardioverter-defibrillator. The importance of this decision reflects the fact that ARVC is a common cause of sudden death in young people and that sudden death may be the first manifestation of the disease. This decision is particularly important because these are often young patients who are expected to live for many years. Although an implantable cardioverter-defibrillator can save lives in individuals with this disease, it is also well recognized that implantable cardioverter-defibrillator therapy is associated with both short- and long-term complications. Decisions about the placement of an implantable cardioverter-defibrillator are based on an estimate of a patient's risk of sudden cardiac death, as well as their preferences and values. The primary purpose of this article is to provide a review of the literature that concerns risk stratification in patients with ARVC and to place this literature in the framework of the 3 authors' considerable lifetime experiences in caring for patients with ARVC. The most important parameters to consider when determining arrhythmic risk include electric instability, including the frequency of premature ventricular contractions and sustained ventricular arrhythmia; proband status; extent of structural disease; cardiac syncope; male sex; the presence of multiple mutations or a mutation in TMEM43; and the patient's willingness to restrict exercise and to eliminate participation in competitive or endurance exercise.
Keywords: arrhythmogenic right ventricular dysplasia; death, sudden, cardiac; defibrillators, implantable; risk assessment; syncope.
© 2017 American Heart Association, Inc.
Conflict of interest statement
Conflict of Interest Disclosure:
Dr Corrado and Dr Marcus have no conflicts of interest to declare.
Figures
References
-
- Marcus FI, Fontaine GH, Guiraudon G, Frank R, Laurenceau JL, Malergue C, Grosgogeat Y. Right ventricular dysplasia: a report of 24 adult cases. Circulation. 1982;65:384–398. - PubMed
-
- Corrado D, Link MS, Calkins H. Arrhythmogenic Right Ventricular Cardiomyopathy. N Engl J Med. 2017;376:61–72. - PubMed
-
- Marcus FI, Fontaine GH, Frank R, Gallagher JJ, Reiter MJ. Long-term follow-up in patients with arrhythmogenic right ventricular disease. Eur Heart J. 1989;10(Supplement D):68–73. - PubMed
-
- Marcus FI. Update of arrhythmogenic right ventricular dysplasia. Card Electrophysiol Rev. 2002;6:54–56. - PubMed
-
- Marcus FI, Abidov A. Arrhythmogenic right ventricular cardiomyopathy 2012: diagnostic challenges and treatment. J Cardiovasc Electrophysiol. 2012;23:1149–1153. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
