

Treatment of Myocardial Infarction with Gene-modified Mesenchymal Stem Cells in a Small Molecular Hydrogel
- PMID: 29158523
- PMCID: PMC5696474
- DOI: 10.1038/s41598-017-15870-z
Treatment of Myocardial Infarction with Gene-modified Mesenchymal Stem Cells in a Small Molecular Hydrogel
Abstract
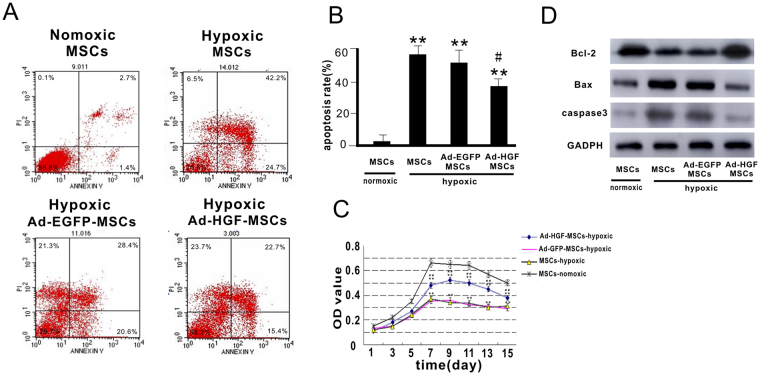
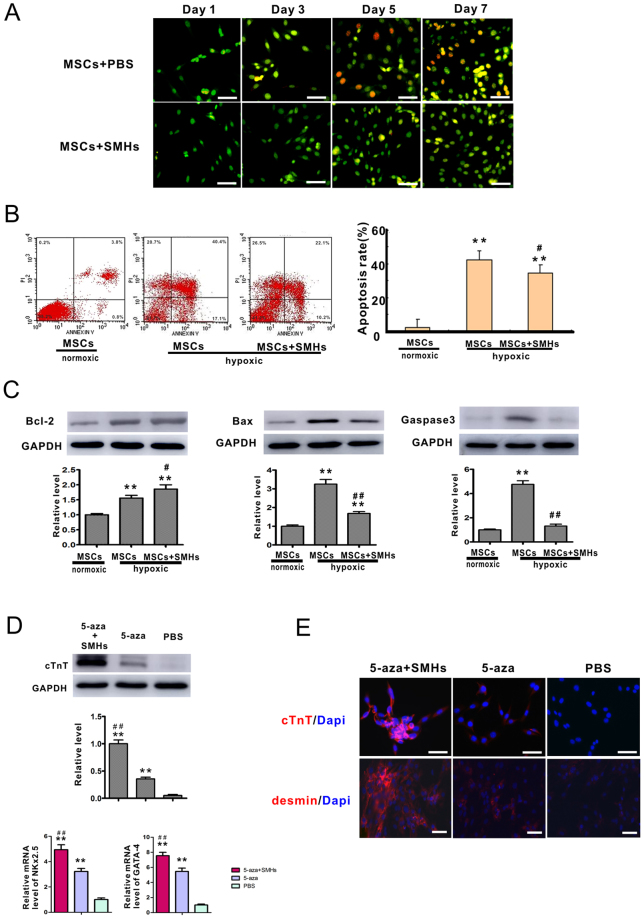
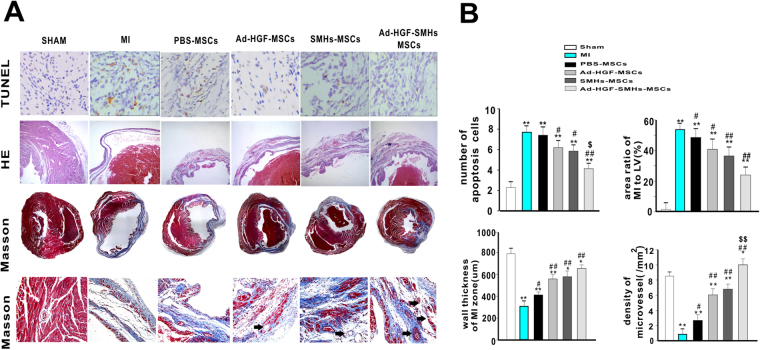
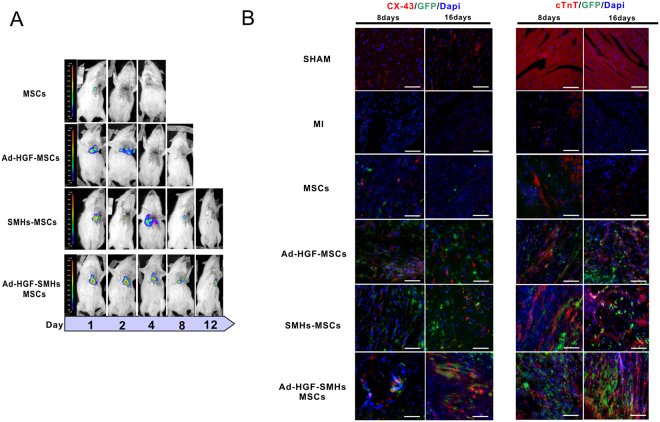
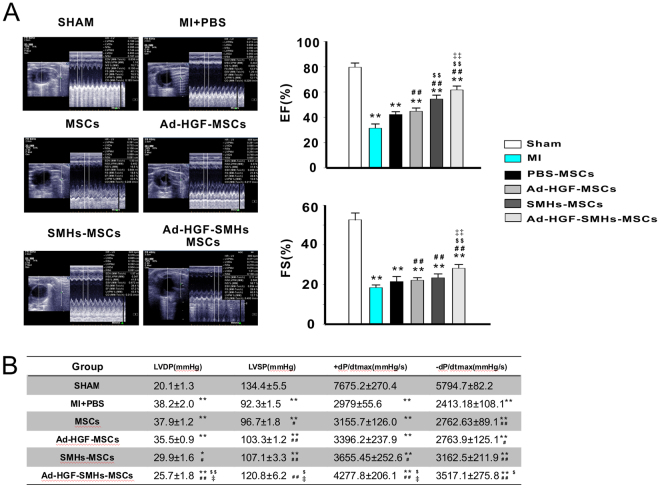
The effect of transplanted rat mesenchymal stem cells (MSCs) can be reduced by extracellular microenvironment in myocardial infarction (MI). We tested a novel small-molecular hydrogel (SMH) on whether it could provide a scaffold for hepatocyte growth factor (HGF)-modified MSCs and alleviate ventricular remodeling while preserving cardiac function after MI. Overexpression of HGF in MSCs increased Bcl-2 and reduced Bax and caspase-3 levels in response to hypoxia in vitro. Immunocytochemistry demonstrated that cardiac troponin (cTnT), desmin and connexin 43 expression were significantly enhanced in the 5-azacytidine (5-aza) with SMH group compared with the 5-aza only group in vitro and in vivo. Bioluminescent imaging indicated that retention and survival of transplanted cells was highest when MSCs transfected with adenovirus (ad-HGF) were injected with SMH. Heart function and structure improvement were confirmed by echocardiography and histology in the Ad-HGF-SMHs-MSCs group compared to other groups. Our study showed that: HGF alleviated cell apoptosis and promoted MSC growth. SMHs improved stem cell adhesion, survival and myocardial cell differentiation after MSC transplantation. SMHs combined with modified MSCs significantly decreased the scar area and improved cardiac function.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Meyer GP, et al. Intracoronary bone marrow cell transfer after myocardial infarction: eighteen months’ follow-up data from the randomized, controlled BOOST (BOne marrOw transfer to enhance ST-elevation infarct regeneration) trial. Circulation. 2006;113:1287–1294. doi: 10.1161/CIRCULATIONAHA.105.575118. - DOI - PubMed
-
- Trachtenberg B, et al. Rationale and design of the Transendocardial Injection of Autologous Human Cells (bone marrow or mesenchymal) in Chronic Ischemic Left Ventricular Dysfunction and Heart Failure Secondary to Myocardial Infarction (TAC-HFT) trial: A randomized, double-blind, placebo-controlled study of safety and efficacy. American heart journal. 2011;161:487–493. doi: 10.1016/j.ahj.2010.11.024. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
