

Evaluation of a deep learning approach for the segmentation of brain tissues and white matter hyperintensities of presumed vascular origin in MRI
- PMID: 29159042
- PMCID: PMC5683197
- DOI: 10.1016/j.nicl.2017.10.007
Evaluation of a deep learning approach for the segmentation of brain tissues and white matter hyperintensities of presumed vascular origin in MRI
Abstract
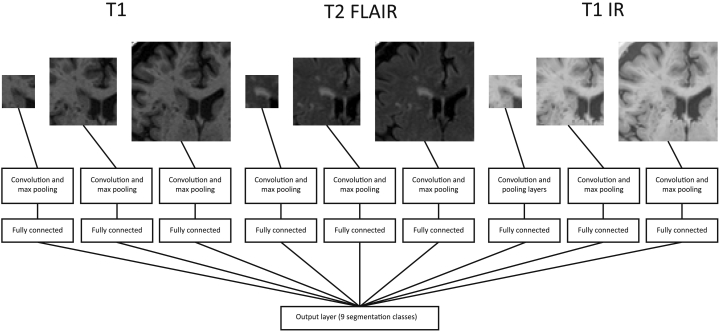
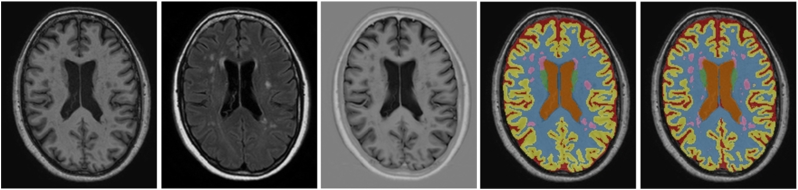
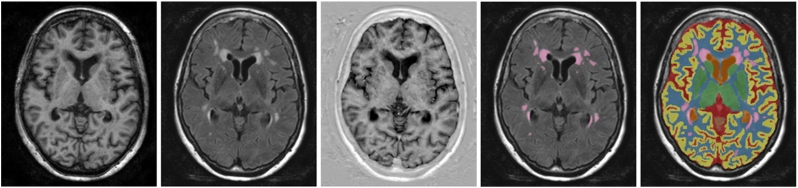
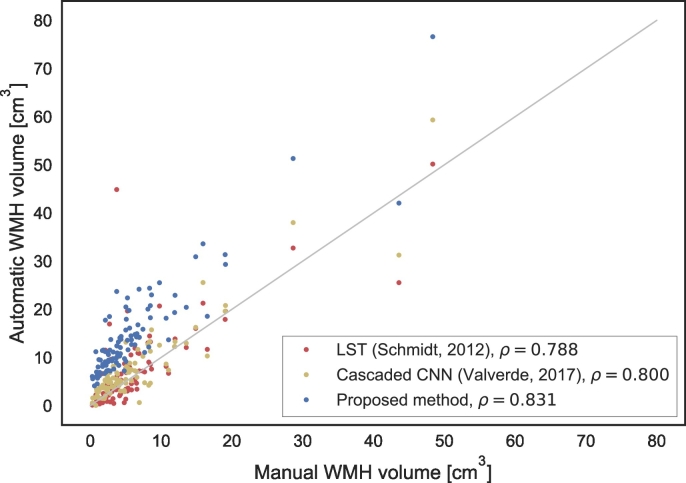
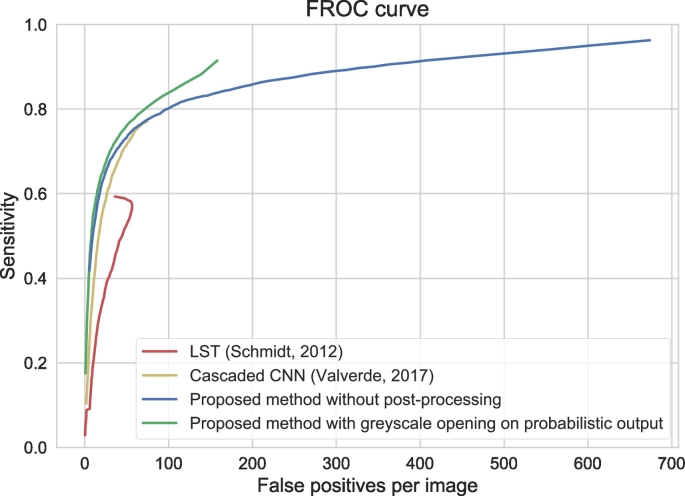
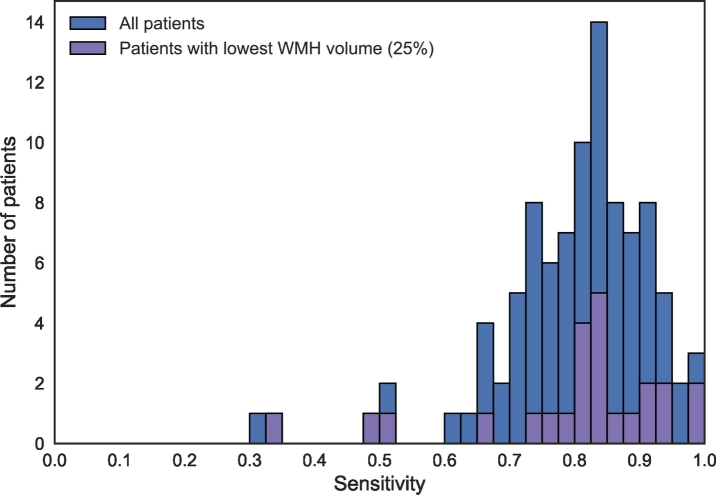
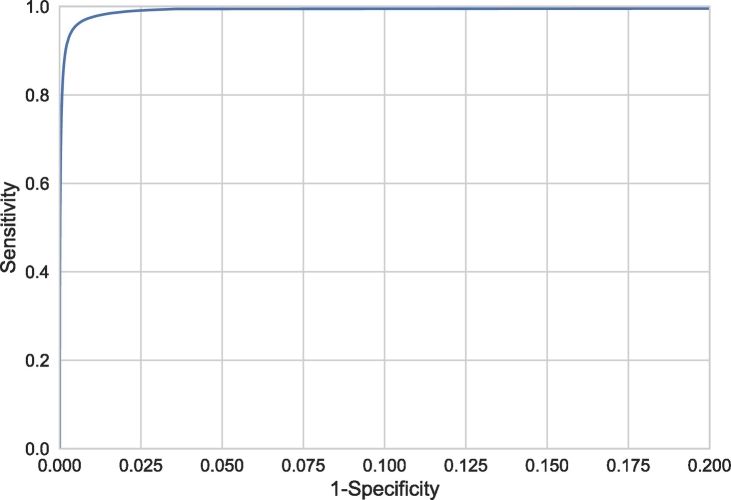
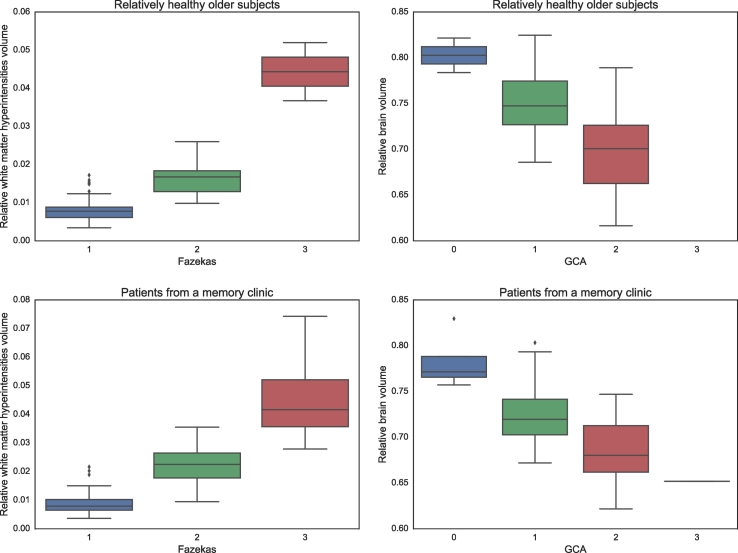
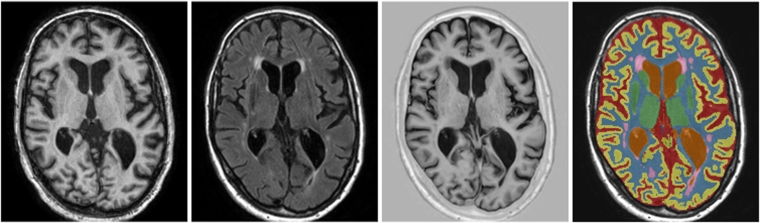
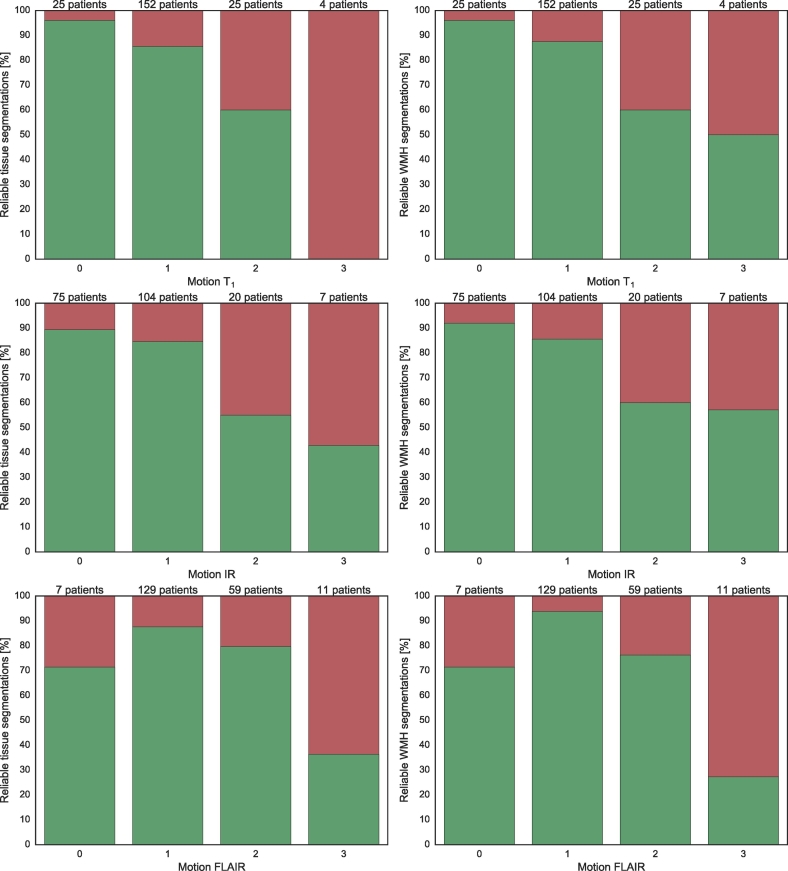
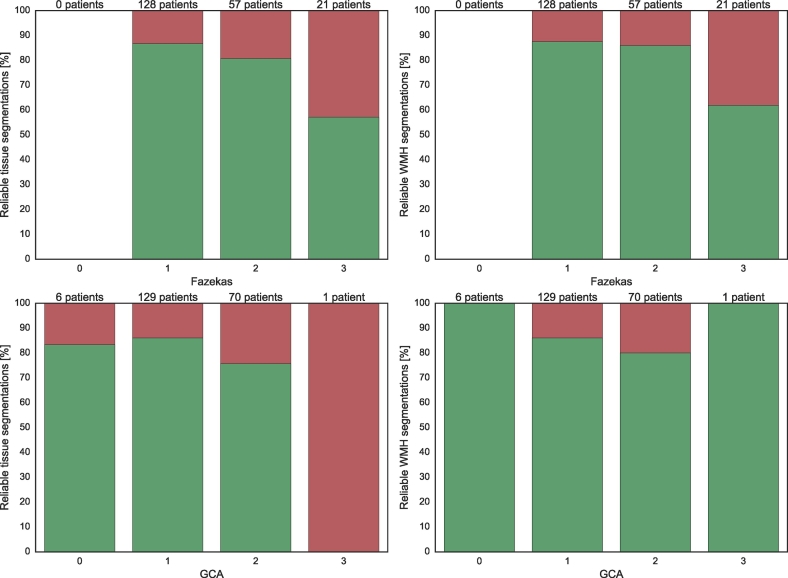
Automatic segmentation of brain tissues and white matter hyperintensities of presumed vascular origin (WMH) in MRI of older patients is widely described in the literature. Although brain abnormalities and motion artefacts are common in this age group, most segmentation methods are not evaluated in a setting that includes these items. In the present study, our tissue segmentation method for brain MRI was extended and evaluated for additional WMH segmentation. Furthermore, our method was evaluated in two large cohorts with a realistic variation in brain abnormalities and motion artefacts. The method uses a multi-scale convolutional neural network with a T1-weighted image, a T2-weighted fluid attenuated inversion recovery (FLAIR) image and a T1-weighted inversion recovery (IR) image as input. The method automatically segments white matter (WM), cortical grey matter (cGM), basal ganglia and thalami (BGT), cerebellum (CB), brain stem (BS), lateral ventricular cerebrospinal fluid (lvCSF), peripheral cerebrospinal fluid (pCSF), and WMH. Our method was evaluated quantitatively with images publicly available from the MRBrainS13 challenge (n = 20), quantitatively and qualitatively in relatively healthy older subjects (n = 96), and qualitatively in patients from a memory clinic (n = 110). The method can accurately segment WMH (Overall Dice coefficient in the MRBrainS13 data of 0.67) without compromising performance for tissue segmentations (Overall Dice coefficients in the MRBrainS13 data of 0.87 for WM, 0.85 for cGM, 0.82 for BGT, 0.93 for CB, 0.92 for BS, 0.93 for lvCSF, 0.76 for pCSF). Furthermore, the automatic WMH volumes showed a high correlation with manual WMH volumes (Spearman's ρ = 0.83 for relatively healthy older subjects). In both cohorts, our method produced reliable segmentations (as determined by a human observer) in most images (relatively healthy/memory clinic: tissues 88%/77% reliable, WMH 85%/84% reliable) despite various degrees of brain abnormalities and motion artefacts. In conclusion, this study shows that a convolutional neural network-based segmentation method can accurately segment brain tissues and WMH in MR images of older patients with varying degrees of brain abnormalities and motion artefacts.
Keywords: Brain MRI; Brain atrophy; Convolutional neural networks; Deep learning; Motion artefacts; Segmentation; White matter hyperintensities.
Figures

Similar articles
-
Automatic segmentation of white matter hyperintensities: validation and comparison with state-of-the-art methods on both Multiple Sclerosis and elderly subjects.Neuroimage Clin. 2022;33:102940. doi: 10.1016/j.nicl.2022.102940. Epub 2022 Jan 10. Neuroimage Clin. 2022. PMID: 35051744 Free PMC article.
-
UBO Detector - A cluster-based, fully automated pipeline for extracting white matter hyperintensities.Neuroimage. 2018 Jul 1;174:539-549. doi: 10.1016/j.neuroimage.2018.03.050. Epub 2018 Mar 22. Neuroimage. 2018. PMID: 29578029
-
Segmentation of white matter hyperintensities using convolutional neural networks with global spatial information in routine clinical brain MRI with none or mild vascular pathology.Comput Med Imaging Graph. 2018 Jun;66:28-43. doi: 10.1016/j.compmedimag.2018.02.002. Epub 2018 Feb 17. Comput Med Imaging Graph. 2018. PMID: 29523002
-
Automatic Detection of White Matter Hyperintensities in Healthy Aging and Pathology Using Magnetic Resonance Imaging: A Review.Neuroinformatics. 2015 Jul;13(3):261-76. doi: 10.1007/s12021-015-9260-y. Neuroinformatics. 2015. PMID: 25649877 Free PMC article. Review.
-
Multi-atlas image registration of clinical data with automated quality assessment using ventricle segmentation.Med Image Anal. 2020 Jul;63:101698. doi: 10.1016/j.media.2020.101698. Epub 2020 Apr 18. Med Image Anal. 2020. PMID: 32339896 Free PMC article. Review.
Cited by
-
Co-optimization Learning Network for MRI Segmentation of Ischemic Penumbra Tissues.Front Neuroinform. 2021 Dec 16;15:782262. doi: 10.3389/fninf.2021.782262. eCollection 2021. Front Neuroinform. 2021. PMID: 34975444 Free PMC article.
-
Diagnostic performance of deep learning-based automatic white matter hyperintensity segmentation for classification of the Fazekas scale and differentiation of subcortical vascular dementia.PLoS One. 2022 Sep 15;17(9):e0274562. doi: 10.1371/journal.pone.0274562. eCollection 2022. PLoS One. 2022. PMID: 36107961 Free PMC article.
-
Utilizing deep learning via the 3D U-net neural network for the delineation of brain stroke lesions in MRI image.Sci Rep. 2023 Nov 13;13(1):19808. doi: 10.1038/s41598-023-47107-7. Sci Rep. 2023. PMID: 37957203 Free PMC article.
-
Ensemble learning via supervision augmentation for white matter hyperintensity segmentation.Front Neurosci. 2022 Sep 15;16:946343. doi: 10.3389/fnins.2022.946343. eCollection 2022. Front Neurosci. 2022. PMID: 36188477 Free PMC article.
-
Changes of the retinal and choroidal vasculature in cerebral small vessel disease.Sci Rep. 2022 Mar 7;12(1):3660. doi: 10.1038/s41598-022-07638-x. Sci Rep. 2022. PMID: 35256658 Free PMC article.
References
-
- Anbeek P., Vincken K.L., van Osch M.J.P., Bisschops R.H.C., van der Grond J. Automatic segmentation of different-sized white matter lesions by voxel probability estimation. Med. Image Anal. 2004;8:205–215. - PubMed
-
- Ashburner J., Friston K.J. Unified segmentation. NeuroImage. 2005;26(3):839–851. - PubMed
-
- Brosch T., Tang L.Y., Yoo Y., Li D.K., Traboulsee A., Tam R. Deep 3D convolutional encoder networks with shortcuts for multiscale feature integration applied to multiple sclerosis lesion segmentation. IEEE Trans. Med. Imaging. 2016;35(5):1229–1239. - PubMed
-
- Brundel M., Reijmer Y.D., van Veluw S.J., Kuijf H.J., Luijten P.R., Kappelle L.J., Biessels G.J. Cerebral microvascular lesions on high-resolution 7-Tesla MRI in patients with type 2 diabetes. Diabetes. 2014;63(10):3523–3529. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
