

PREP2: A biomarker-based algorithm for predicting upper limb function after stroke
- PMID: 29159193
- PMCID: PMC5682112
- DOI: 10.1002/acn3.488
PREP2: A biomarker-based algorithm for predicting upper limb function after stroke
Abstract
Objective: Recovery of motor function is important for regaining independence after stroke, but difficult to predict for individual patients. Our aim was to develop an efficient, accurate, and accessible algorithm for use in clinical settings. Clinical, neurophysiological, and neuroimaging biomarkers of corticospinal integrity obtained within days of stroke were combined to predict likely upper limb motor outcomes 3 months after stroke.
Methods: Data from 207 patients recruited within 3 days of stroke [103 females (50%), median age 72 (range 18-98) years] were included in a Classification and Regression Tree analysis to predict upper limb function 3 months poststroke.
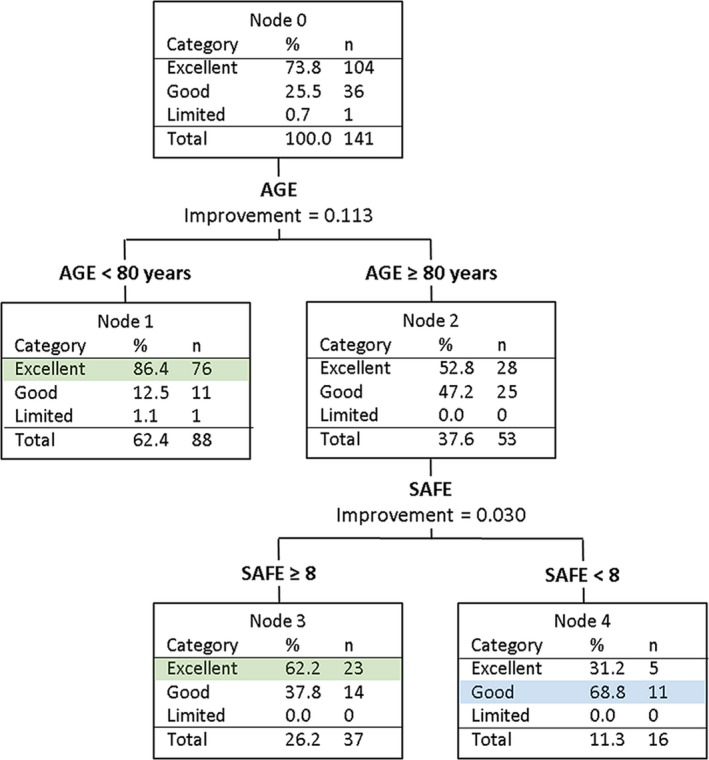
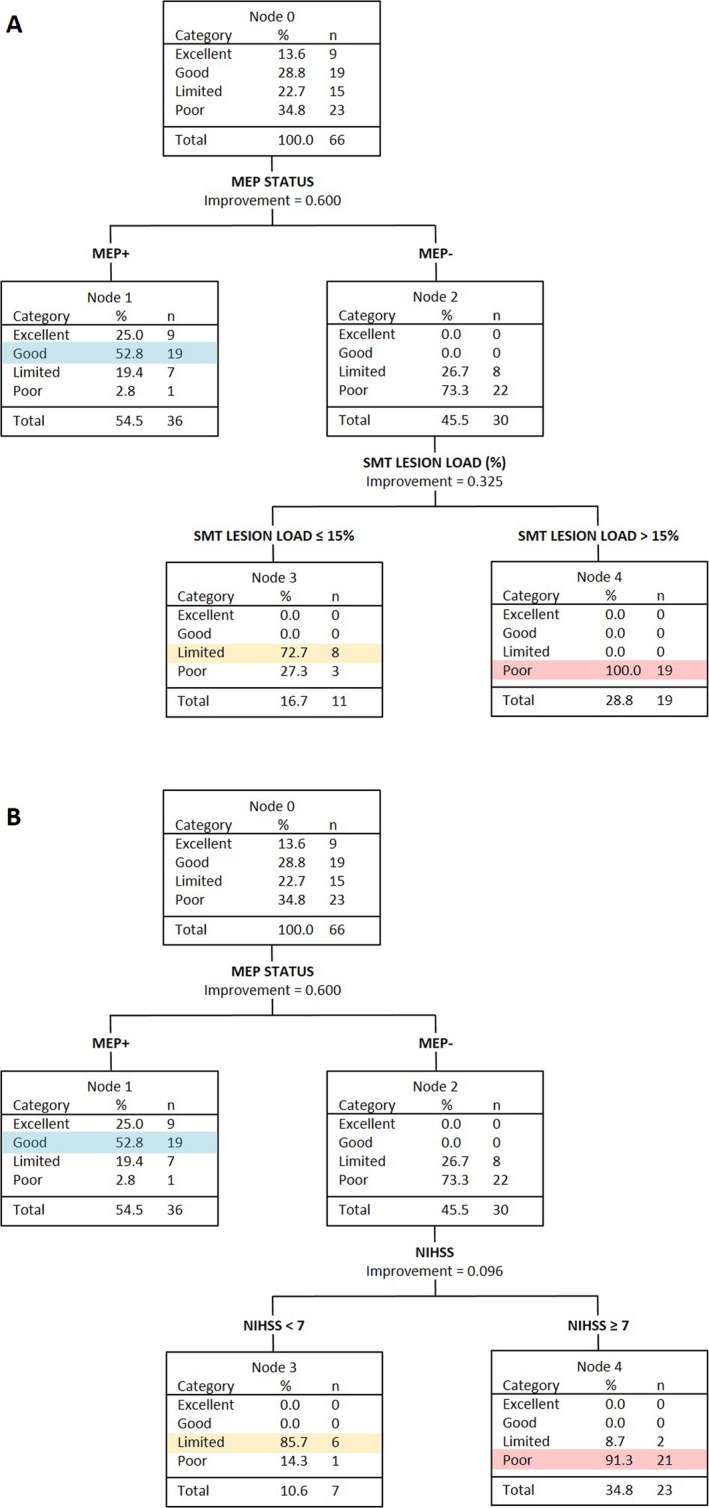
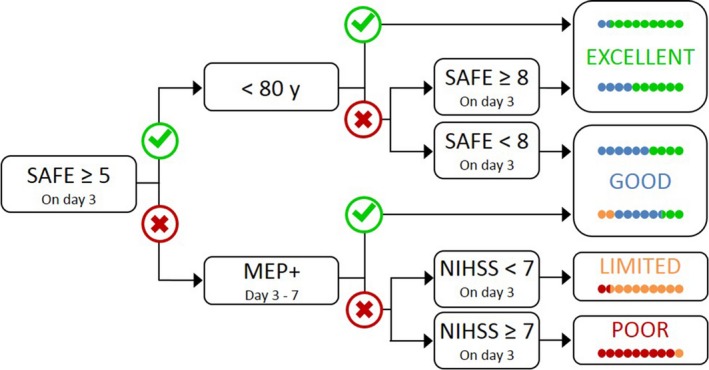
Results: The analysis produced an algorithm that sequentially combined a measure of upper limb impairment; age; the presence or absence of upper limb motor evoked potentials elicited with transcranial magnetic stimulation; and stroke lesion load obtained from MRI or stroke severity assessed with the NIHSS score. The algorithm makes correct predictions for 75% of patients. A key biomarker obtained with transcranial magnetic stimulation is required for one third of patients. This biomarker combined with NIHSS score can be used in place of more costly magnetic resonance imaging, with no loss of prediction accuracy.
Interpretation: The new algorithm is more accurate, efficient, and accessible than its predecessors, which may support its use in clinical practice. While further work is needed to potentially incorporate sensory and cognitive factors, the algorithm can be used within days of stroke to provide accurate predictions of upper limb functional outcomes at 3 months after stroke. www.presto.auckland.ac.nz.
Figures
References
-
- Langhorne P, Coupar F, Pollock A. Motor recovery after stroke: a systematic review. Lancet Neurol 2009;8:741–754. - PubMed
-
- Veerbeek JM, Kwakkel G, van Wegen EE, et al. Early prediction of outcome of activities of daily living after stroke: a systematic review. Stroke 2011;42:1482–1488. - PubMed
-
- Coupar F, Pollock A, Rowe P, et al. Predictors of upper limb recovery after stroke: a systematic review and meta‐analysis. Clin Rehabil 2012;26:291–313. - PubMed
-
- Nijland RH, van Wegen EE, Harmeling‐van der Wel BC, et al. Accuracy of physical therapists’ early predictions of upper‐limb function in hospital stroke units: the EPOS study. Phys Ther 2013;93:460–469. - PubMed
-
- Stinear CM, Byblow WD, Ackerley SJ, et al. Predicting recovery potential for individual stroke patients increases rehabilitation efficiency. Stroke 2017;48:1011–1019. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
