

Prospective comparison of novel dark blood late gadolinium enhancement with conventional bright blood imaging for the detection of scar
- PMID: 29162123
- PMCID: PMC5696884
- DOI: 10.1186/s12968-017-0407-x
Prospective comparison of novel dark blood late gadolinium enhancement with conventional bright blood imaging for the detection of scar
Abstract
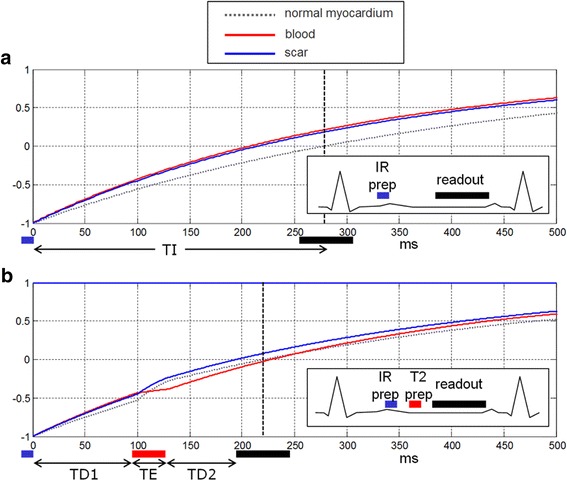
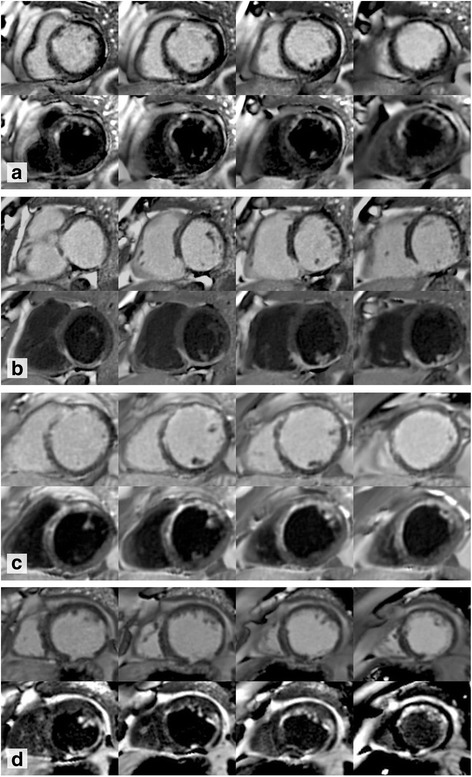
Background: Conventional bright blood late gadolinium enhancement (bright blood LGE) imaging is a routine cardiovascular magnetic resonance (CMR) technique offering excellent contrast between areas of LGE and normal myocardium. However, contrast between LGE and blood is frequently poor. Dark blood LGE (DB LGE) employs an inversion recovery T2 preparation to suppress the blood pool, thereby increasing the contrast between the endocardium and blood. The objective of this study is to compare the diagnostic utility of a novel DB phase sensitive inversion recovery (PSIR) LGE CMR sequence to standard bright blood PSIR LGE.
Methods: One hundred seventy-two patients referred for clinical CMR were scanned. A full left ventricle short axis stack was performed using both techniques, varying which was performed first in a 1:1 ratio. Two experienced observers analyzed all bright blood LGE and DB LGE stacks, which were randomized and anonymized. A scoring system was devised to quantify the presence and extent of gadolinium enhancement and the confidence with which the diagnosis could be made.
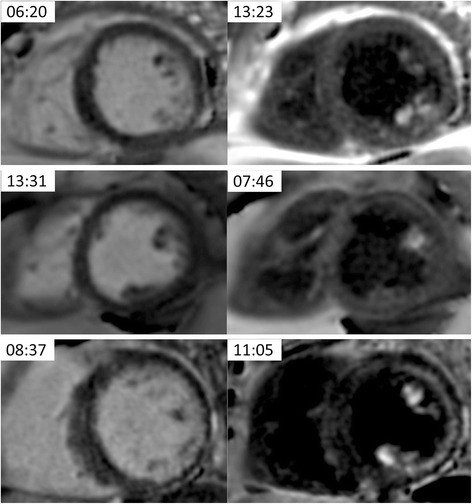
Results: A total of 2752 LV segments were analyzed. There was very good inter-observer correlation for quantifying LGE. DB LGE analysis found 41.5% more segments that exhibited hyperenhancement in comparison to bright blood LGE (248/2752 segments (9.0%) positive for LGE with bright blood; 351/2752 segments (12.8%) positive for LGE with DB; p < 0.05). DB LGE also allowed observers to be more confident when diagnosing LGE (bright blood LGE high confidence in 154/248 regions (62.1%); DB LGE in 275/324 (84.9%) regions (p < 0.05)). Eighteen patients with no bright blood LGE were found to have had DB LGE, 15 of whom had no known history of myocardial infarction.
Conclusions: DB LGE significantly increases LGE detection compared to standard bright blood LGE. It also increases observer confidence, particularly for subendocardial LGE, which may have important clinical implications.
Keywords: Bright blood; Dark blood; Inversion recovery; Late gadolinium enhancement; Myocardial infarction; PSIR.
Conflict of interest statement
Ethics approval and consent to participate
All ethics were approved by the UCL/UCLH Joint Committees on the Ethics of Human Research Committee, and all participants provided written informed consent.
Consent for publication
Written informed consent was obtained from patients for publication of their individual details and accompanying images in this manuscript. The consent form is held on record and is available for review by the Editor-in-Chief.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- Burns RJ, Gibbons RJ, Yi Q, Roberts RS, Miller TD, Schaer GL, et al. The relationships of left ventricular ejection fraction, end-systolic volume index and infarct size to six-month mortality after hospital discharge following myocardial infarction treated by thrombolysis. J Am Coll Cardiol. 2002;39(1):30–36. doi: 10.1016/S0735-1097(01)01711-9. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
