

Managing toxicities associated with immune checkpoint inhibitors: consensus recommendations from the Society for Immunotherapy of Cancer (SITC) Toxicity Management Working Group
- PMID: 29162153
- PMCID: PMC5697162
- DOI: 10.1186/s40425-017-0300-z
Managing toxicities associated with immune checkpoint inhibitors: consensus recommendations from the Society for Immunotherapy of Cancer (SITC) Toxicity Management Working Group
Abstract
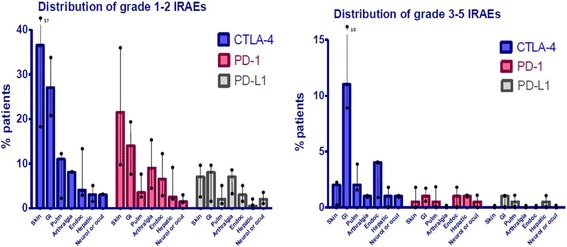
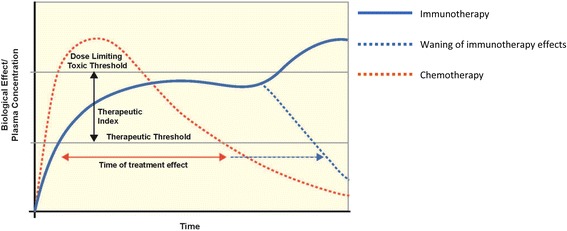
Cancer immunotherapy has transformed the treatment of cancer. However, increasing use of immune-based therapies, including the widely used class of agents known as immune checkpoint inhibitors, has exposed a discrete group of immune-related adverse events (irAEs). Many of these are driven by the same immunologic mechanisms responsible for the drugs' therapeutic effects, namely blockade of inhibitory mechanisms that suppress the immune system and protect body tissues from an unconstrained acute or chronic immune response. Skin, gut, endocrine, lung and musculoskeletal irAEs are relatively common, whereas cardiovascular, hematologic, renal, neurologic and ophthalmologic irAEs occur much less frequently. The majority of irAEs are mild to moderate in severity; however, serious and occasionally life-threatening irAEs are reported in the literature, and treatment-related deaths occur in up to 2% of patients, varying by ICI. Immunotherapy-related irAEs typically have a delayed onset and prolonged duration compared to adverse events from chemotherapy, and effective management depends on early recognition and prompt intervention with immune suppression and/or immunomodulatory strategies. There is an urgent need for multidisciplinary guidance reflecting broad-based perspectives on how to recognize, report and manage organ-specific toxicities until evidence-based data are available to inform clinical decision-making. The Society for Immunotherapy of Cancer (SITC) established a multidisciplinary Toxicity Management Working Group, which met for a full-day workshop to develop recommendations to standardize management of irAEs. Here we present their consensus recommendations on managing toxicities associated with immune checkpoint inhibitor therapy.
Keywords: Immune checkpoint inhibitor; Immune-related adverse events; Toxicity.
Conflict of interest statement
Authors information
Dr. Abdallah participated in this workshop while employed by AstraZeneca, Gaithersburg, MD but has since moved to Merck & Co., Inc.
Dr. Lenihan participated in this workshop while employed at Vanderbilt University Medical Center, Nashville, TN, but has since moved to Washington University in St Louis, St Louis, MO.
Competing interests
AF declared that he is an employee of Gritstone Oncology, Inc. BP declared that he is an employee and shareholder of Merck & Co., Inc. CS declared that she is a member of Genentech, Inc. Tecentriq Speakers Bureau. CR declared that she received personal fees through service on the advisory boards at Bristol-Myers Squibb Co., GlaxoSmithKline Pharmaceuticals Ltd., Novartis International AG, Amgen, Inc., Merck & Co., Inc., and F. Hoffmann-La Roche, Ltd. DC declared that he was employed by Genentech, Inc., until June 2016. DJL declared that he has received personal compensation as a consultant for F. Hoffmann-La Roche, Ltd., Bristol-Myers Squibb Co., and Amgen, Inc., and research support from Takeda Pharmaceuticals U.S.A., Inc. DT declared that she is an employee and shareholder of Pfizer, Inc. DW declared that he has been an employee and shareholder of Janssen Research & Development, LLC, from May 2016, to present, and an employee of Bayer Healthcare Pharmaceuticals, Inc., from June 2012, to May 2016. IP declared that he received consulting fees from Amgen, Inc., and F. Hoffmann-La Roche, Ltd. JR declared that she is a research nurse at Johns Hopkins University and works with patients receiving IO agents from multiple sponsors and investigator-initiated studies; JR has also participated in Institute for Clinical Immuno-Oncology Immunotherapy Workshops, has participated in reviewing educational materials developed by AstraZeneca committee and an advisory board meeting sponsored by Merck EMD. JS declared that she is an employee of AstraZeneca Pharmaceuticals. KA declared that he was an employee of AstraZeneca Pharmaceuticals until May 2015, is currently an employee and shareholder of Merck & Co., Inc., and is a shareholder of Sanofi. KS-W declared that she is an employee of AstraZeneca Pharmaceuticals. MD declared that she has a financial relationship with Speakers Bureau: AstraZeneca Pharmaceuticals; Genentech, Inc.; Merck & Co., Inc.; Bristol-Myers Squibb Co. ML declared that he has received personal fees from Quintiles Inc., Janssen Research & Development, LLC, AstraZeneca Pharmaceuticals, Genentech, Inc., Foamix Pharmaceuticals Inc., Infinity Pharmaceuticals, Adgero Biopharmaceuticals Holdings, Inc., Bristol-Myers Squibb Co., and Berg LLC. MS declared that he is an employee of AstraZeneca Pharmaceuticals. MS-A declared that she participated in the Bristol-Myers Squibb Co Advisory Board. OL declared that he has financial relationships with Bristol-Myers Squibb Co, MSD (Merck & Co., Inc.) and Janssen Research & Development, LLC. RD Declared that she receives personal fees from serving on the advisory board at Bristol-Myers Squibb Co. SA declared that she has a financial relationship with Genentech, Inc. Speaker’s Bureau. SL declared that he was an employee of Janssen Research & Development, LLC until January 2016, and is currently an employee of Genentech, Inc. VH declared that she is an employee of AstraZeneca Pharmaceuticals. WS declared that he received consulting fees and general funding from Merck & Co., Inc., Bristol-Myers Squibb Co, and Novartis International AG. ZR declared that he is an employee of AstraZeneca Pharmaceuticals. All remaining authors declared no competing interests.
Figures
References
-
- Administration, U.S.F.a.D. Drugs@FDA: FDA approved drug products. 2017 June 19th, 2017]; Available from: https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm.
-
- Company, B.-M.S. Ipilimumab (Yervoy) Highlights of Prescribing Information. 2017 3/2017 [cited 2017 June 19th, 2017]; Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2015/125377s073lbl.pdf.
-
- Company, B.-M.S. Nivolumab (Opdivo) Highlights of Prescribing Information. 2017 4/2017 [cited 2017 June 19th, 2017]; Available from: https://packageinserts.bms.com/pi/pi_opdivo.pdf.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous