

Predicting Outcome in Patients with Anti-GBM Glomerulonephritis
- PMID: 29162595
- PMCID: PMC5753308
- DOI: 10.2215/CJN.04290417
Predicting Outcome in Patients with Anti-GBM Glomerulonephritis
Abstract
Background and objectives: Large studies on long-term kidney outcome in patients with anti-glomerular basement membrane (anti-GBM) GN are lacking. This study aimed to identify clinical and histopathologic parameters that predict kidney outcome in these patients.
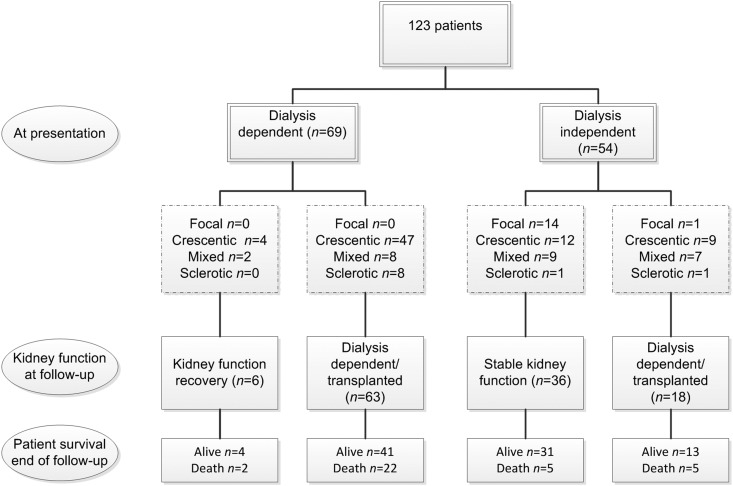
Design, setting, participants, & measurements: This retrospective analysis included a total of 123 patients with anti-GBM GN between 1986 and 2015 from six centers worldwide. Their kidney biopsy samples were classified according to the histopathologic classification for ANCA-associated GN. Clinical data such as details of treatment were retrieved from clinical records. The primary outcome parameter was the occurrence of ESRD. Kidney survival was analyzed using the log-rank test and Cox regression analyses.
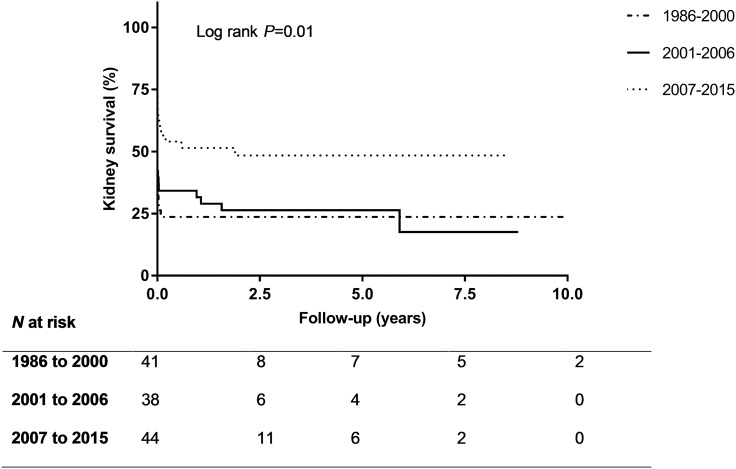
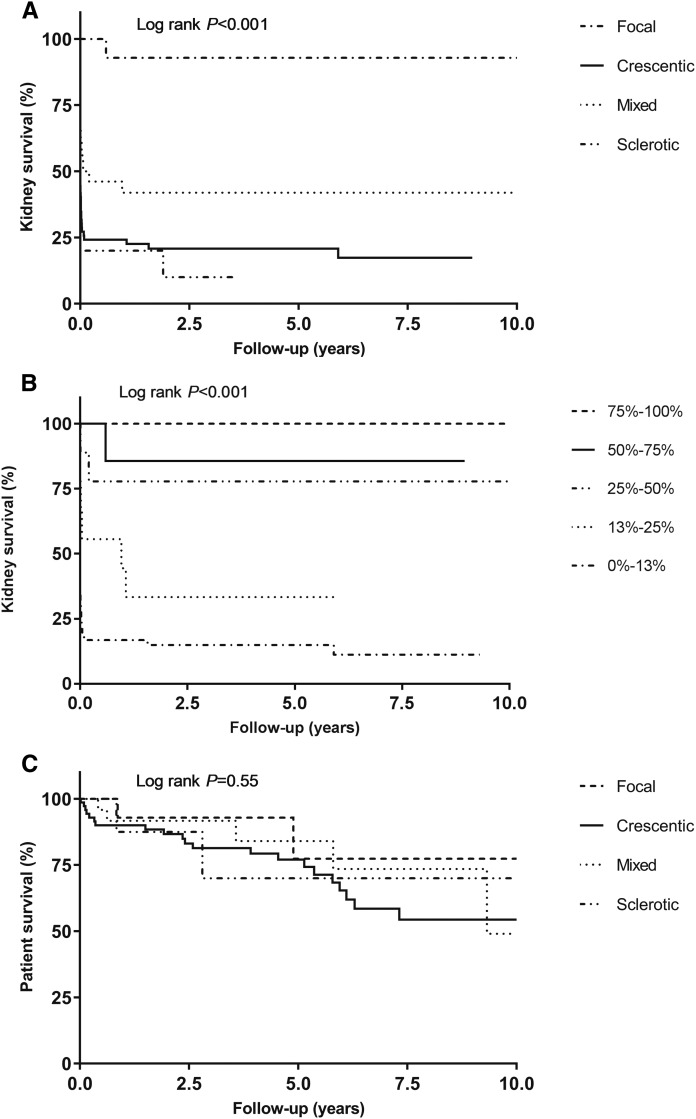
Results: The 5-year kidney survival rate was 34%, with an improved rate observed among patients diagnosed after 2007 (P=0.01). In patients with anti-GBM GN, histopathologic class and kidney survival were associated (P<0.001). Only one of 15 patients with a focal class biopsy sample (≥50% normal glomeruli) developed ESRD. Patients with a sclerotic class biopsy sample (≥50% globally sclerotic glomeruli) and patients with 100% cellular crescents did not recover from dialysis dependency at presentation. In multivariable analysis, dialysis dependency at presentation (hazard ratio [HR], 3.17; 95% confidence interval [95% CI], 1.59 to 6.32), percentage of normal glomeruli (HR, 0.97; 95% CI, 0.95 to 0.99), and extent of interstitial infiltrate (HR, 2.02; 95% CI, 1.17 to 3.50) were predictors of ESRD during follow-up.
Conclusions: Dialysis dependency, low percentage of normal glomeruli, and large extent of interstitial infiltrate are associated with poor kidney outcome in anti-GBM GN. Kidney outcome has improved during recent years; the success rate doubled after 2007.
Podcast: This article contains a podcast at https://www.asn-online.org/media/podcast/CJASN/2017_11_21_CJASNPodcast_18_1_v.mp3.
Keywords: ANCA; Antibodies, Antineutrophil Cytoplasmic; Autoantibodies; Biopsy; Confidence Intervals; Follow-Up Studies; Glomerular Basement Membrane; Goodpasture-s syndrome; Kidney Failure, Chronic; Multivariate Analysis; Regression Analysis; Retrospective Studies; Survival Rate; anti-GBM disease; antiglomerular basement membrane antibody; glomerulonephritis; kidney; kidney biopsy; renal dialysis.
Copyright © 2018 by the American Society of Nephrology.
Figures
Comment in
- 1–2 doi: 10.2215/CJN.13211117
References
-
- Jennette JC, Falk RJ, Bacon PA, Basu N, Cid MC, Ferrario F, Flores-Suarez LF, Gross WL, Guillevin L, Hagen EC, Hoffman GS, Jayne DR, Kallenberg CG, Lamprecht P, Langford CA, Luqmani RA, Mahr AD, Matteson EL, Merkel PA, Ozen S, Pusey CD, Rasmussen N, Rees AJ, Scott DG, Specks U, Stone JH, Takahashi K, Watts RA: 2012 revised international chapel hill consensus conference nomenclature of vasculitides. Arthritis Rheum 65: 1–11, 2013 - PubMed
-
- Canney M, O’Hara PV, McEvoy CM, Medani S, Connaughton DM, Abdalla AA, Doyle R, Stack AG, O’Seaghdha CM, Clarkson MR, Griffin MD, Holian J, Dorman AM, Niland A, Keogan M, Wallace EM, Conlon NP, Walsh C, Kelly A, Little MA: Spatial and temporal clustering of anti-glomerular basement membrane disease. Clin J Am Soc Nephrol 11: 1392–1399, 2016 - PMC - PubMed
-
- Jennette JC: Rapidly progressive crescentic glomerulonephritis. Kidney Int 63: 1164–1177, 2003 - PubMed
-
- Chang A: Anti-GBM glomerulonephritis. In: Diagnostic Pathology: Kidney Diseases, 2nd Ed., Philadelphia, PA, Elsevier Health Sciences, 2015
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
