

CD4+ T Cells Orchestrate Lethal Immune Pathology despite Fungal Clearance during Cryptococcus neoformans Meningoencephalitis
- PMID: 29162707
- PMCID: PMC5698549
- DOI: 10.1128/mBio.01415-17
CD4+ T Cells Orchestrate Lethal Immune Pathology despite Fungal Clearance during Cryptococcus neoformans Meningoencephalitis
Abstract
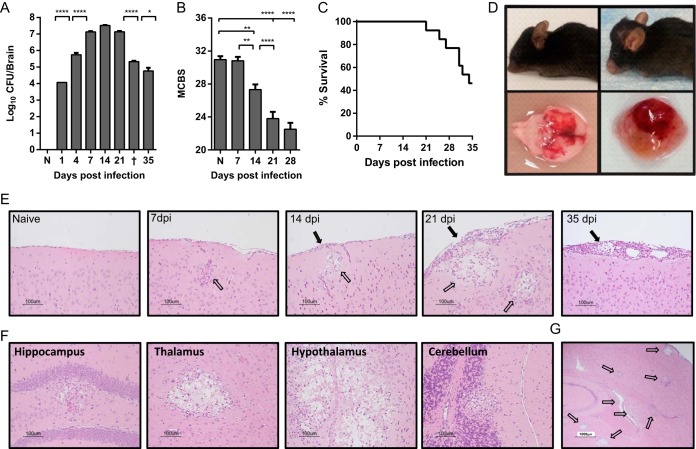
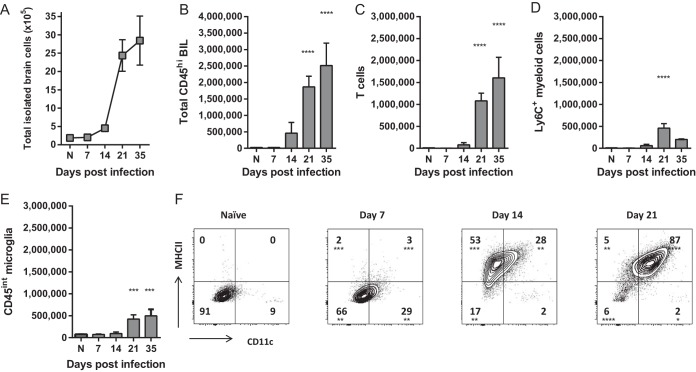
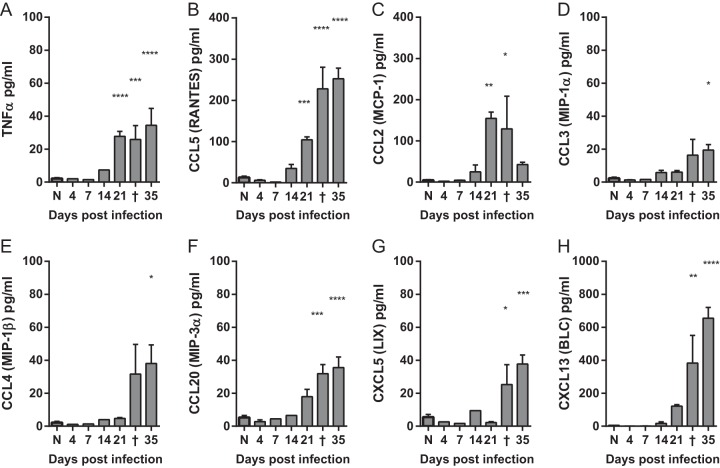
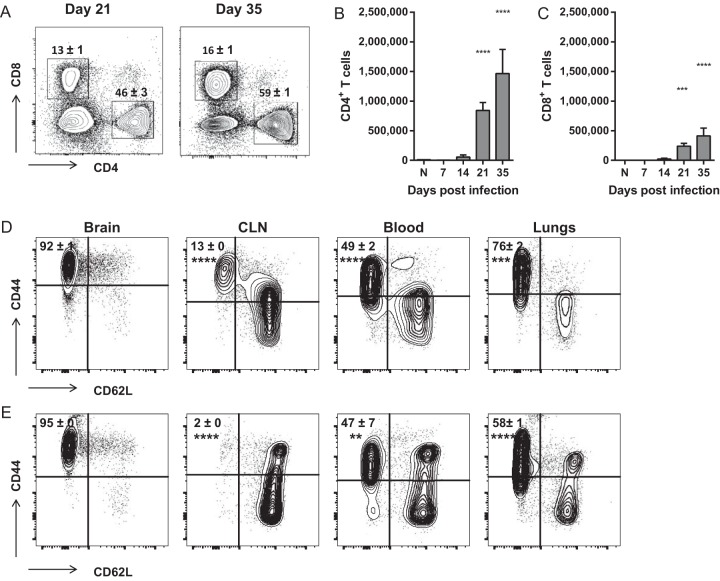
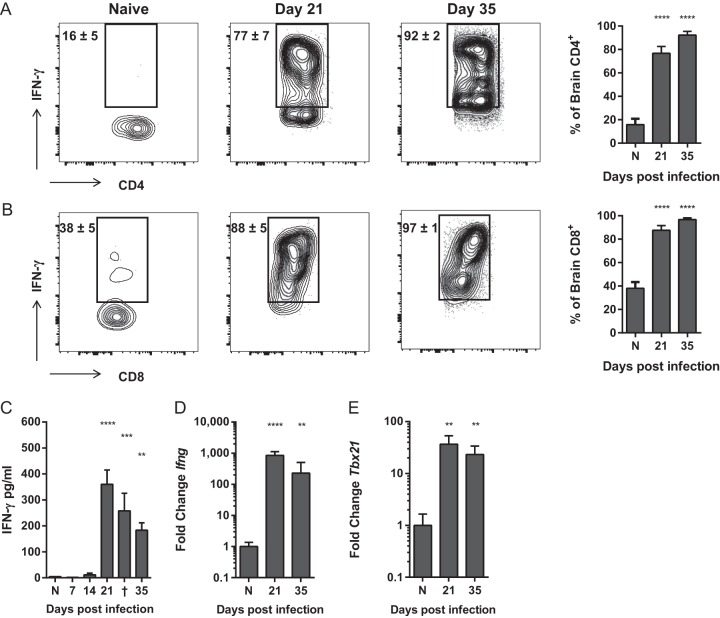
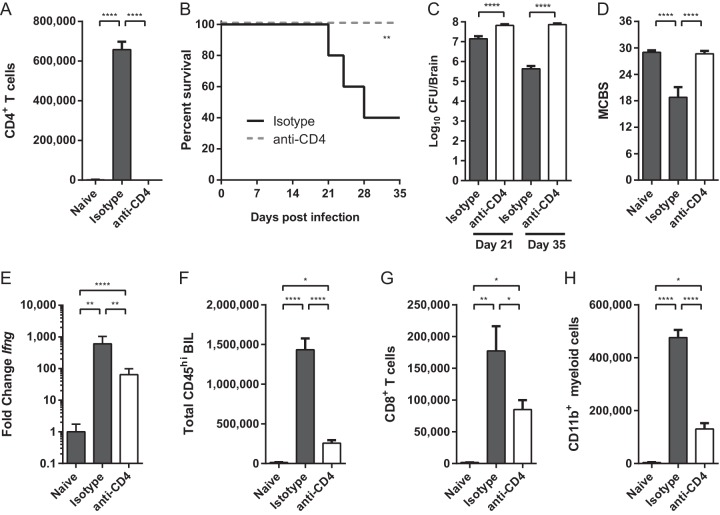
Cryptococcus neoformans is a major fungal pathogen that disseminates to the central nervous system (CNS) to cause fatal meningoencephalitis, but little is known about immune responses within this immune-privileged site. CD4+ T cells have demonstrated roles in anticryptococcal defenses, but increasing evidence suggests that they may contribute to clinical deterioration and pathology in both HIV-positive (HIV+) and non-HIV patients who develop immune reconstitution inflammatory syndrome (IRIS) and post-infectious inflammatory response syndrome (PIIRS), respectively. Here we report a novel murine model of cryptococcal meningoencephalitis and a potential damaging role of T cells in disseminated cryptococcal CNS infection. In this model, fungal burdens plateaued in the infected brain by day 7 postinfection, but activation of microglia and accumulation of CD45hi leukocytes was significantly delayed relative to fungal growth and did not peak until day 21. The inflammatory leukocyte infiltrate consisted predominantly of gamma interferon (IFN-γ)-producing CD4+ T cells, conventionally believed to promote fungal clearance and recovery. However, more than 50% of mice succumbed to infection and neurological dysfunction between days 21 and 35 despite a 100-fold reduction in fungal burdens. Depletion of CD4+ cells significantly impaired IFN-γ production, CD8+ T cell and myeloid cell accumulation, and fungal clearance from the CNS but prevented the development of clinical symptoms and mortality. These findings conclusively demonstrate that although CD4+ T cells are necessary to control fungal growth, they can also promote significant immunopathology and mortality during CNS infection. The results from this model may provide important guidance for development and use of anti-inflammatory therapies to minimize CNS injury in patients with severe cryptococcal infections.IMPORTANCE CNS infection with the fungal pathogen Cryptococcus neoformans often results in debilitating brain injury and has a high mortality rate despite antifungal treatment. Treatment is complicated by the fact that immune responses needed to eliminate infection are also thought to drive CNS damage in a subset of both HIV+ and non-HIV patients. Thus, physicians need to balance efforts to enhance patients' immune responses and promote microbiological control with anti-inflammatory therapy to protect the CNS. Here we report a novel model of cryptococcal meningoencephalitis demonstrating that fungal growth within the CNS does not immediately cause symptomatic disease. Rather, accumulation of antifungal immune cells critically mediates CNS injury and mortality. This model demonstrates that antifungal immune responses in the CNS can cause detrimental pathology and addresses the urgent need for animal models to investigate the specific cellular and molecular mechanisms underlying cryptococcal disease in order to better treat treat patients with CNS infections.
Keywords: Cryptococcus; Cryptococcus neoformans; IRIS; PIIRS; T cells; central nervous system infections; encephalitis; fungi; immunopathology; meningitis; opportunistic infections.
Figures
Comment in
-
Immune-Mediated Damage Completes the Parabola: Cryptococcus neoformans Pathogenesis Can Reflect the Outcome of a Weak or Strong Immune Response.mBio. 2017 Dec 12;8(6):e02063-17. doi: 10.1128/mBio.02063-17. mBio. 2017. PMID: 29233901 Free PMC article.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
