

Quality of antenatal care service provision in health facilities across sub-Saharan Africa: Evidence from nationally representative health facility assessments
- PMID: 29163936
- PMCID: PMC5680531
- DOI: 10.7189/jogh.07.021101
Quality of antenatal care service provision in health facilities across sub-Saharan Africa: Evidence from nationally representative health facility assessments
Abstract
Background: Utilization of antenatal care (ANC) services has increased over the past two decades. Continued gains in maternal and newborn health will require an understanding of both access and quality of ANC services. We linked health facility and household survey data to examine the quality of service provision for five ANC interventions across health facilities in sub-Saharan Africa.
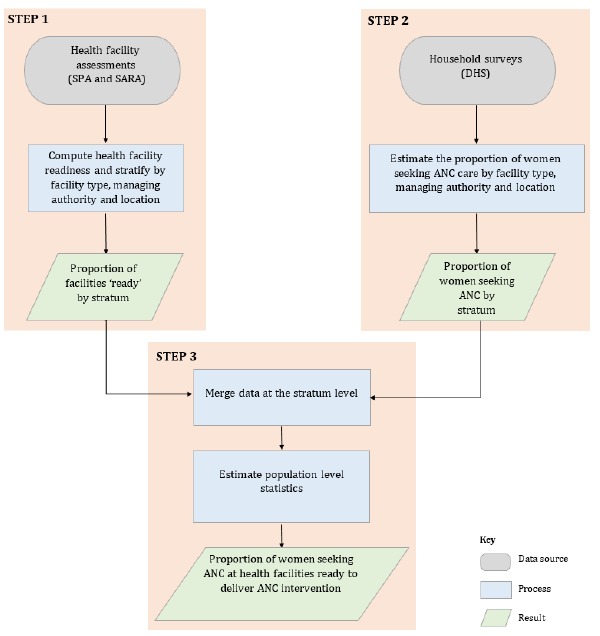
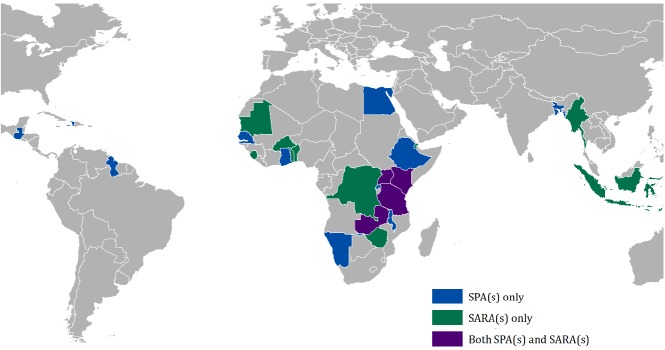
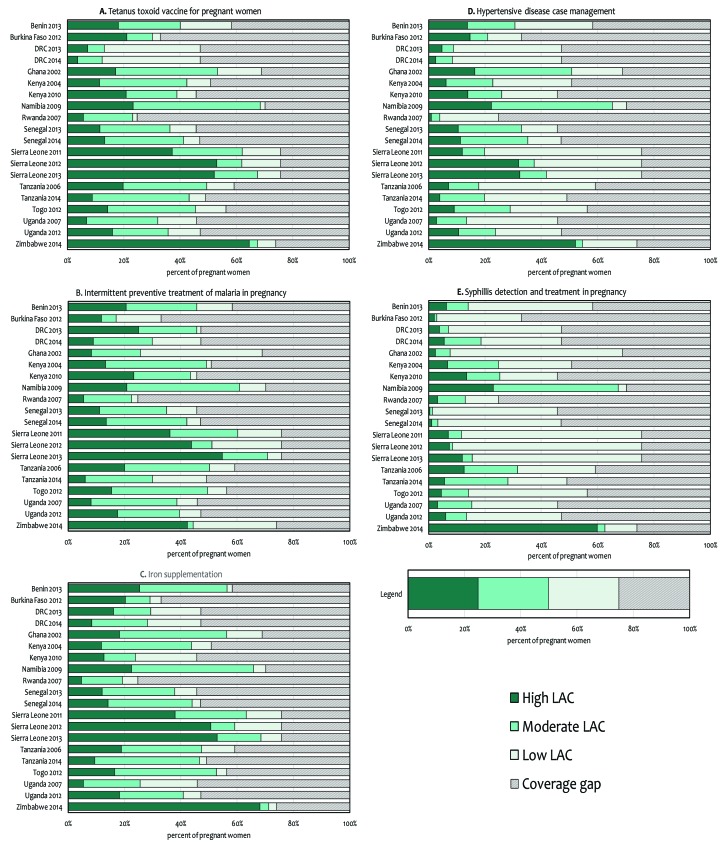
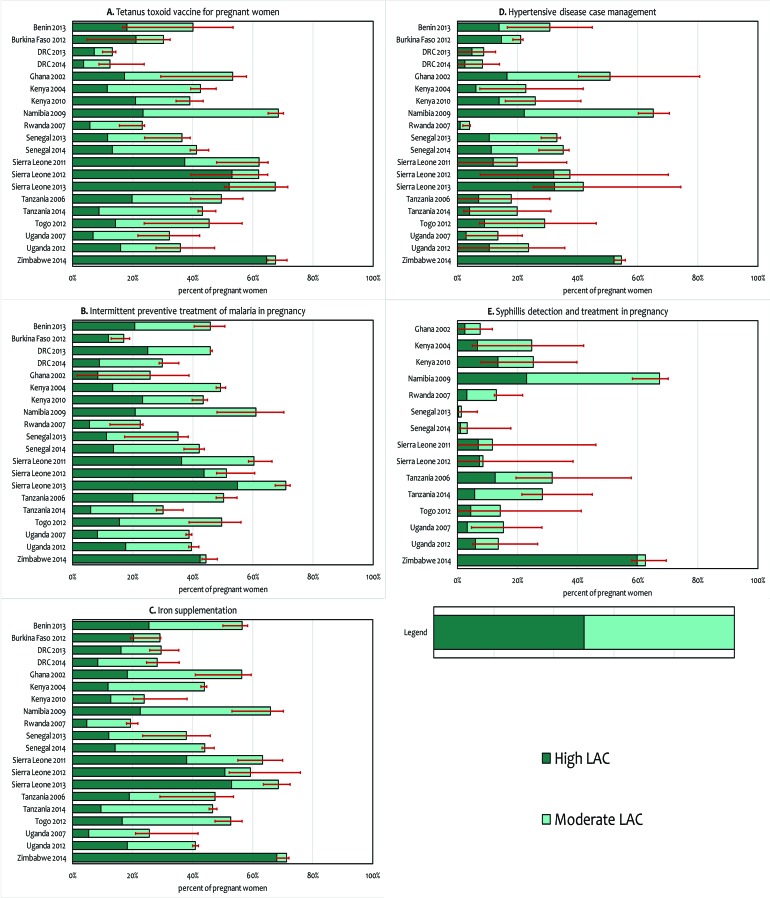
Methods: Using data from 20 nationally representative health facility assessments - the Service Provision Assessment (SPA) and the Service Availability and Readiness Assessment (SARA), we estimated facility level readiness to deliver five ANC interventions: tetanus toxoid vaccine for pregnant women, intermittent preventive treatment for malaria in pregnancy (IPTp), syphilis detection and treatment in pregnancy, iron supplementation and hypertensive disease case management. Facility level indicators were stratified by health facility type, managing authority and location, then linked to estimates of ANC utilization in that stratum from the corresponding Demographic and Health Surveys (DHS) to generate population level estimates of the 'likelihood of appropriate care'. Finally, the association between estimates of the 'likelihood of appropriate care' from the linking approach and estimates of coverage levels from the DHS were assessed.
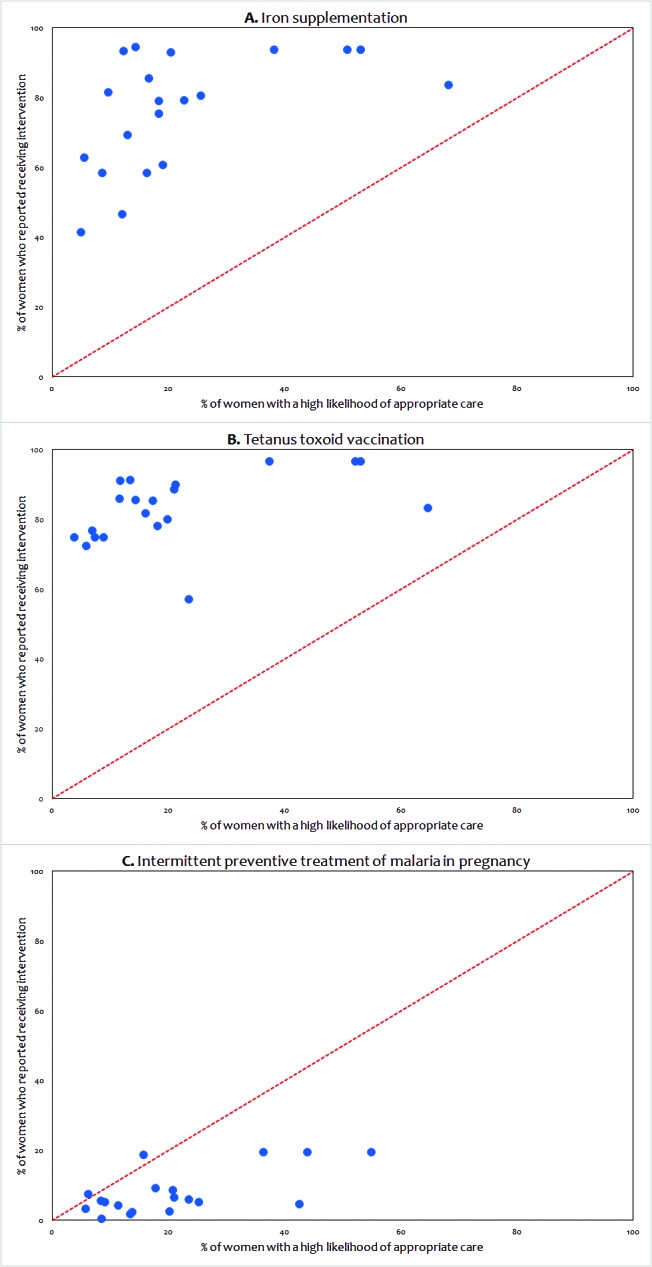
Findings: A total of 10 534 health facilities were surveyed in the 20 health facility assessments, of which 8742 reported offering ANC services and were included in the analysis. Health facility readiness to deliver IPTp, iron supplementation, and tetanus toxoid vaccination was higher (median: 84.1%, 84.9% and 82.8% respectively) than readiness to deliver hypertensive disease case management and syphilis detection and treatment (median: 23.0% and 19.9% respectively). Coverage of at least 4 ANC visits ranged from 24.8% to 75.8%. Estimates of the likelihood of appropriate care derived from linking health facility and household survey data showed marked gaps for all interventions, particularly hypertensive disease case management and syphilis detection and treatment. There was fairly good concordance between our estimates of high likelihood of appropriate care and DHS estimates of coverage for iron supplementation, IPTp, and tetanus toxoid vaccination.
Conclusion: Linking household surveys to health facility assessments revealed marked gaps in population-level coverage of quality ANC interventions and underscored the need for a double-pronged approach to increase ANC utilization and improve the quality of ANC services.
Conflict of interest statement
Competing interests: The authors have completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare no conflicts of interests.
Figures
References
-
- Indicators for monitoring the Millennium Development Goals: definitions, rationale, concepts and sources. United Nations Publications; Available:http://mdgs.un.org/unsd/mi/wiki/MainPage.ashx. Accessed 10 September 2016.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
