

Timing of Decompression in Patients With Acute Spinal Cord Injury: A Systematic Review
- PMID: 29164038
- PMCID: PMC5684838
- DOI: 10.1177/2192568217701716
Timing of Decompression in Patients With Acute Spinal Cord Injury: A Systematic Review
Abstract
Study design: Systematic review.
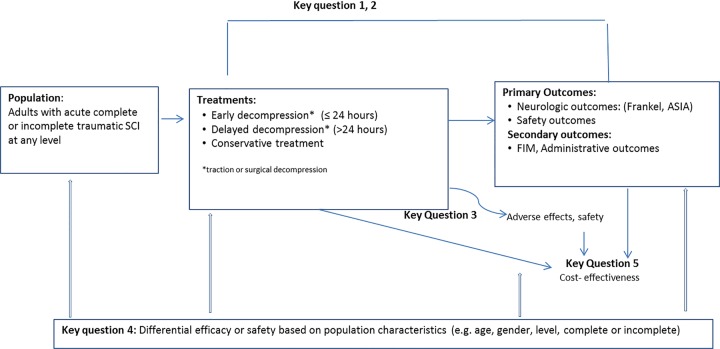
Objective: To conduct a systematic review and synthesis of the literature to assess the comparative effectiveness, safety, and cost-effectiveness of early (≤24 hours) versus late decompression (>24 hours) in adults with acute spinal cord injury (SCI).
Methods: A systematic search was conducted of Medline, EMBASE, the Cochrane Collaboration Library, and Google Scholar to identify studies published through November 6, 2014. Studies published in any language, in humans, and with an abstract were considered for inclusion. Included studies were critically appraised and the overall strength of evidence was determined using methods proposed by the Grading of Recommendation Assessment, Development and Evaluation working group.
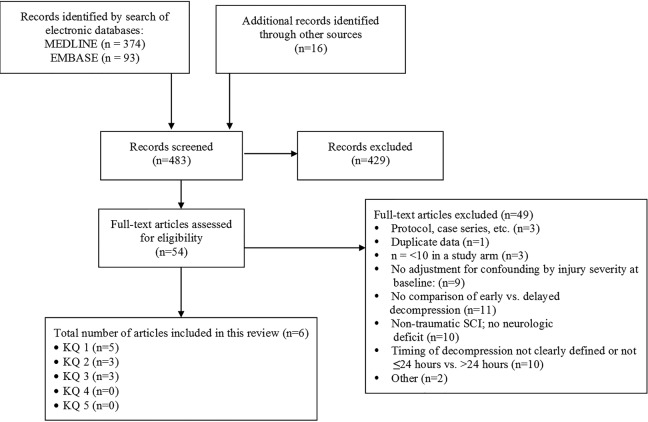
Results: The search yielded 449 potentially relevant citations. Sixteen additional primary studies were identified through other sources. Six studies met inclusion criteria. All but 2 studies were considered to have moderately high risk of bias. Across studies and injury levels, the impact of early surgical decompression (≤24 hours) on clinically important improvement in neurological status was variable. Isolated studies reported statistically significant and clinically important improvements at 6 months (cervical injury, low strength of evidence) and following discharge from inpatient rehabilitation (all levels, very low strength of evidence) but not at other time points; another study observed a statistically significant 6 point improvement in ASIA Impairment Scale (AIS) among patients with AIS B, C, or D, but not for those with AIS A (very low strength of evidence). In one study of acute central cord syndrome without instability, a clinically and statistically meaningful improvement in total motor scores was reported at 6 and 12 months in patients treated early (versus late). There were, however, no significant differences in AIS improvement between early and late surgical groups at 6- or 12-months (very low strength of evidence). One of 3 studies found a shorter length of hospital stay associated with early surgical decompression. Of 3 studies reporting on safety, no significant differences in rates of complications (including mortality, neurologic deterioration, pneumonia or pressure ulcers) were noted between early and late decompression groups.
Conclusions: Results surrounding the efficacy of early versus late decompressive surgery, as well as the quality of evidence available, were variable depending on the level of SCI, timing of follow-up, and specific outcome considered. Existing evidence supports improved neurological recovery among cervical SCI patients undergoing early surgery; however, evidence regarding remaining SCI populations and clinical outcomes was inconsistent.
Keywords: spinal cord injury; systematic review; timing of surgery.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Rowland J, Hawryluk G, Kwon B, Fehlings MG. Current status of acute spinal cord injury pathophysiology and emerging therapies: promise on the horizon. Neurosurg Focus. 2008;25:E2. - PubMed
-
- Hawryluk G, Roland J, Kwon B, Fehlings M. Protection and repair of the injured spinal cord: a review of completed, ongoing, and planned clinical trials for acute spinal cord injury. Neurosurg Focus. 2008;25:E14. - PubMed
-
- Guha A, Tator C, Endrenyi L. Decompression of the spinal cord improves recovery after acute experimental spinal cord compression injury. Paraplegia. 1987;25:324–339. - PubMed
-
- Dimar J, Glassman S, Raque G, Zhang YP, Shields CB. The influence of spinal canal narrowing and timing of decompression on neurologic recovery after spinal cord contusion in a rat model. Spine (Phila Pa 1976). 1999;24:1623–1633. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
