

Acute Septic Arthritis of the Knee Caused by Kingella kingae in a 5-Year-Old Cameroonian Boy
- PMID: 29164082
- PMCID: PMC5681518
- DOI: 10.3389/fped.2017.00230
Acute Septic Arthritis of the Knee Caused by Kingella kingae in a 5-Year-Old Cameroonian Boy
Abstract
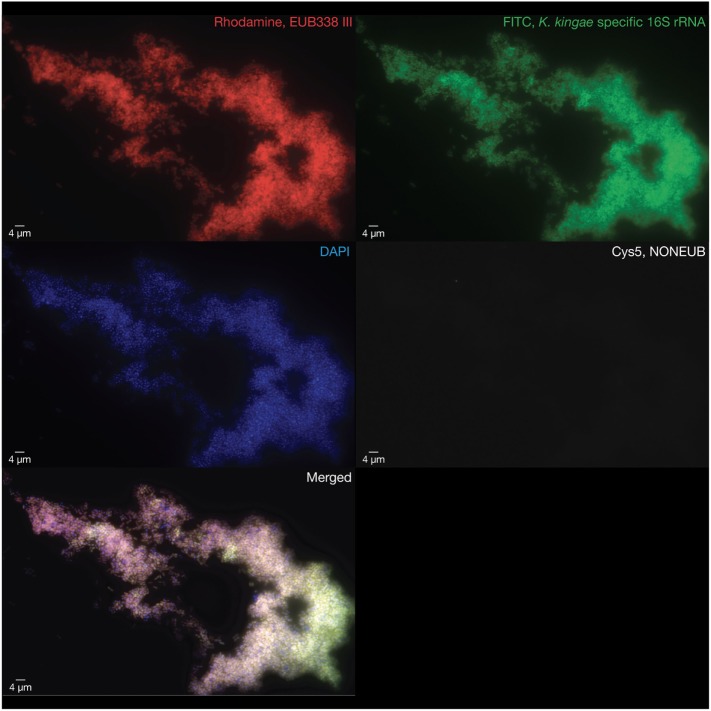
Kingella kingae is an important cause of invasive infections in young children from Western countries. Although increasing reports indicate that this organism is the leading agent of bone and joint infections in early childhood, data on K. kingae infections from resource-limited settings are scarce, and none has yet been reported in Africa. We herein report the diagnostic and epidemiological investigations of the first case of K. kingae arthritis identified in a child from sub-Saharan Africa. A 5-year-old Cameroonian boy presented with a sudden painful limp which appeared in the course of a mild rhinopharyngitis. He lived in Cameroon where he had been vaccinated with BCG at birth and moved to France for holidays 4 days before consultation. There was no history of trauma and he did not have any underlying medical condition. Upon admission, he had a temperature of 36.7°C, and clinical examination revealed right-sided knee tenderness and effusion that was confirmed by ultrasound imaging. Laboratory results showed a white blood cell count of 5,700 cells/mm3, C-reactive protein level of 174 mg/L, and platelet count of 495,000 cells/mm3. He underwent an arthrocentesis and was immediately given intravenous amoxicillin-clavulanate. Conventional cultures from blood samples and synovial fluids were negative. Polymerase chain reaction (PCR) assay targeting the broad-range 16S rRNA gene and real-time quantitative PCR assays targeting Mycobacterium species were negative. Surprisingly, real-time PCR assays targeting the cpn60, rtxA, and rtxB genes of K. kingae were positive. Multicolor fluorescence in situ hybridization specific for K. kingae identified the presence of numerous coccobacilli located within the synovial fluid. Finally, multilocus sequence typing analysis performed on deoxyribonucleic acid directly extracted from joint fluid disclosed a novel K. kingae sequence-type complex. This case report demonstrates that K. kingae may be considered as a potential cause of septic arthritis in children living in sub-Saharan Africa, and hence the burden of K. kingae infection may be not limited to the Western countries. Further studies are required to determine the prevalence of K. kingae infection and carriage in Africa.
Keywords: Africa South of the Sahara; Kingella kingae; arthritis; infectious; multilocus sequence typing; pediatrics.
Figures
References
-
- Ceroni D, Llana RA, Kherad O, Dubois-Ferriere V, Lascombes P, Renzi G, et al. Comparing the oropharyngeal colonization density of Kingella kingae between asymptomatic carriers and children with invasive osteoarticular infections. Pediatr Infect Dis J (2013) 32:412–4. 10.1097/INF.0b013e3182846e8f - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials