

Continuous Laparoscopic Closure of the Linea Alba with Barbed Sutures Combined with Laparoscopic Mesh Implantation (IPOM Plus Repair) As a New Technique for Treatment of Abdominal Hernias
- PMID: 29164131
- PMCID: PMC5676438
- DOI: 10.3389/fsurg.2017.00062
Continuous Laparoscopic Closure of the Linea Alba with Barbed Sutures Combined with Laparoscopic Mesh Implantation (IPOM Plus Repair) As a New Technique for Treatment of Abdominal Hernias
Abstract
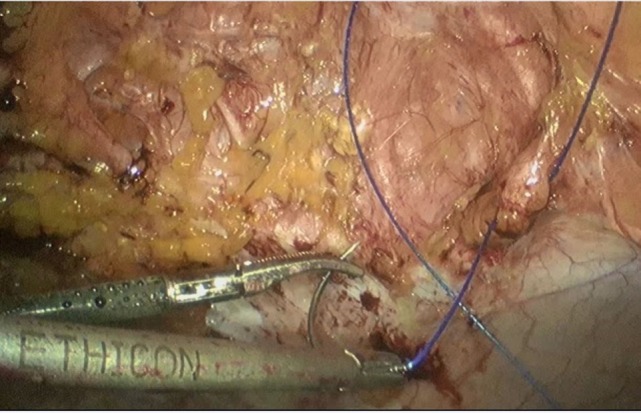
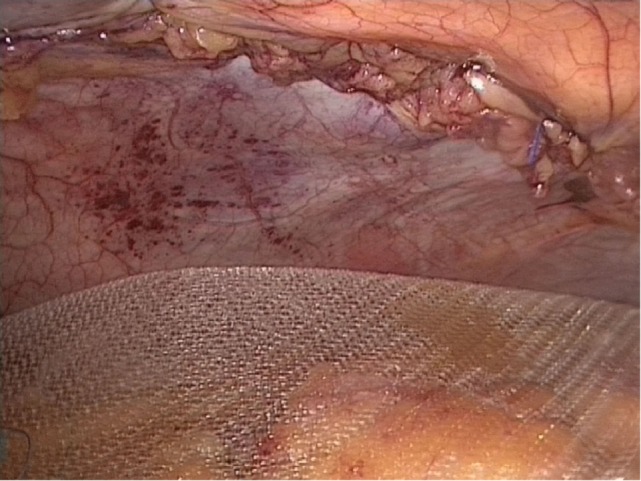
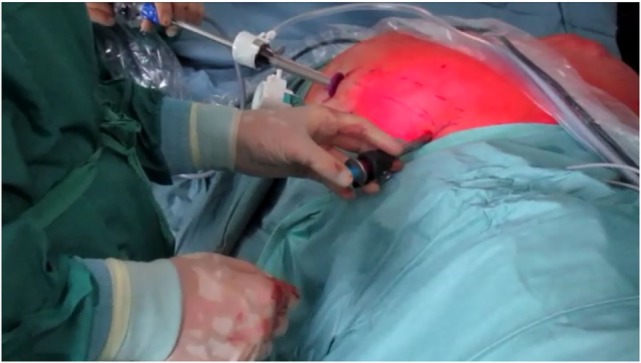
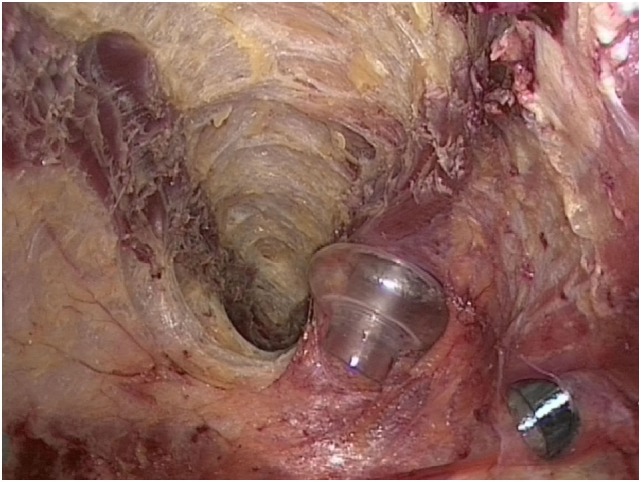
Despite extensive experience and significant reduction of complications in recent years, laparoscopic treatment of complex abdominal hernias is a challenge even for the experienced endoscopic surgeon. Patients with severe incisional hernias or symptomatic rectus diastasis benefit from the closure of the linea alba as a morphological and physiological reconstruction of the abdominal wall followed by mesh implantation. Occasionally, an additional component separation is necessary. In open surgery, this is associated with very large wound areas, postoperative seromas, poor wound healing and, in the worst case, mesh infections. To avoid these complications, we operate these complex reconstructions completely endoscopically. Our concept is based on a laparoscopic closure of the linea alba through an ongoing, barbed non-resorbable 1-0 suture (polybutester) and final reinforcement by an intraperitoneal-onlay mesh (IPOM-Plus). For the treatment of complex abdominal hernias with a width of more than 10 cm, we performed an endoscopic anterior bilateral component separation. This allows the surgeon to combine the advantages of the open abdominal wall reconstruction with those of laparoscopic hernia repair. Between May 2015 and June 2017, we treated 42 patients with abdominal hernias by laparoscopic continuous hernia defect closure and complementary mesh implantation, whereby a complex reconstruction with additional endoscopic anterior component separation was performed in five patients. In this article, we will present this innovative technique of endoscopic/laparoscopic hernia repair in complex abdominal hernias.
Keywords: IPOMplus; abdominal Hernia; barbed suture; laparoscopic component separation.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous