

AIDS-Related Endemic Mycoses in Western Cape, South Africa, and Clinical Mimics: A Cross-Sectional Study of Adults With Advanced HIV and Recent-Onset, Widespread Skin Lesions
- PMID: 29164168
- PMCID: PMC5695619
- DOI: 10.1093/ofid/ofx186
AIDS-Related Endemic Mycoses in Western Cape, South Africa, and Clinical Mimics: A Cross-Sectional Study of Adults With Advanced HIV and Recent-Onset, Widespread Skin Lesions
Abstract
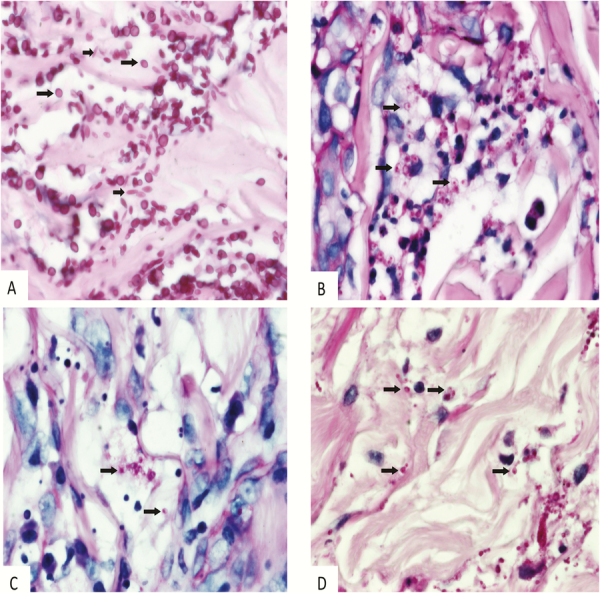
Background: Skin lesions are common in advanced HIV infection and are sometimes caused by serious diseases like systemic mycoses (SM). AIDS-related SM endemic to Western Cape, South Africa, include emergomycosis (formerly disseminated emmonsiosis), histoplasmosis, and sporotrichosis. We previously reported that 95% of patients with AIDS-related emergomycosis had skin lesions, although these were frequently overlooked or misdiagnosed clinically. Prospective studies are needed to characterize skin lesions of SM in South Africa and to help distinguish these from common HIV-related dermatoses.
Methods: We prospectively enrolled HIV-infected adult patients living in Western Cape, South Africa, with CD4 counts ≤100 cells/μL and widespread skin lesions present ≤6 months that were deemed clinically compatible with SM. We obtained skin biopsies for histopathology and fungal culture and collected epidemiological and clinical data.
Results: Of 34 patients enrolled and in whom a diagnosis could be made, 25 had proven SM: 14 had emergomycosis, and 3 each had histoplasmosis and sporotrichosis; for 5 additional patients, the fungal species could not be identified. Antiretroviral therapy (ART) had been initiated in the preceding 4 weeks for 11/25 (44%) patients with SM (vs no patients without SM). Plaques and scale crust occurred more frequently in patients with SM (96% vs 25%, P = .0002; and 67% vs 13%, P = .01, respectively).
Conclusions: Recent ART initiation and presence of plaques or scale crust should make clinicians consider SM in patients with advanced HIV infection in this geographic area. Clinical overlap between SM and other dermatoses makes early skin biopsy critical for timely diagnosis and treatment.
Keywords: Emergomyces africanus; emergomycosis; emmonsiosis; histoplasmosis; sporotrichosis.
Figures

References
-
- Coldiron BM, Bergstresser PR, Farthling CF et al. . Prevalence and clinical spectrum of skin disease in patients infected with human immunodeficiency virus. Arch Dermatol 1989; 125:357–61. - PubMed
-
- Amerson EH, Maurer TA. Dermatologic manifestations of HIV in Africa. Top HIV Med 2010; 18:16–22. - PubMed
-
- Tschachler E, Bergstresser PR, Stingl G. HIV-related skin diseases. Lancet 1996; 348:659–63. - PubMed
-
- Tsang MW, Kovarik CL. Global access to dermatopathology services: physician survey of availability and needs in sub-Saharan Africa. J Am Acad Dermatol 2010; 63:346–8. - PubMed
-
- Motswaledi MH, Visser W. The spectrum of HIV-associated infective and inflammatory dermatoses in pigmented skin. Dermatol Clin 2014; 32:211–25. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
