

Prevalence of Pre-Diabetes across Ethnicities: A Review of Impaired Fasting Glucose (IFG) and Impaired Glucose Tolerance (IGT) for Classification of Dysglycaemia
- PMID: 29165385
- PMCID: PMC5707745
- DOI: 10.3390/nu9111273
Prevalence of Pre-Diabetes across Ethnicities: A Review of Impaired Fasting Glucose (IFG) and Impaired Glucose Tolerance (IGT) for Classification of Dysglycaemia
Abstract
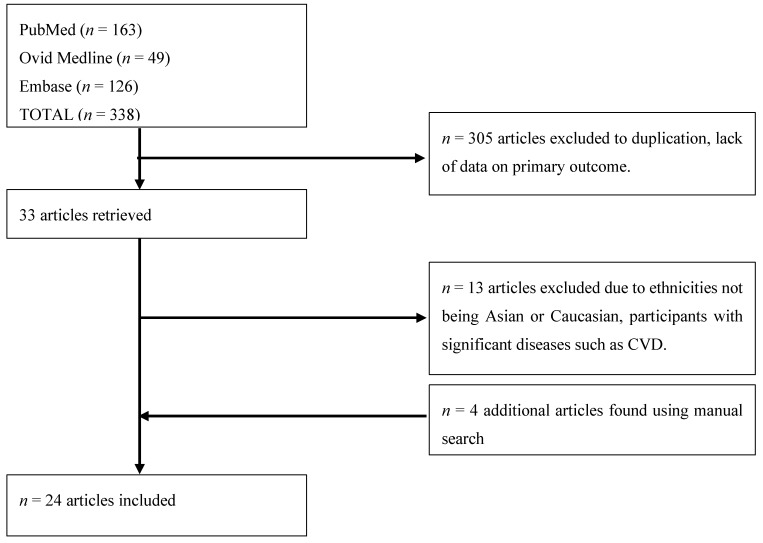
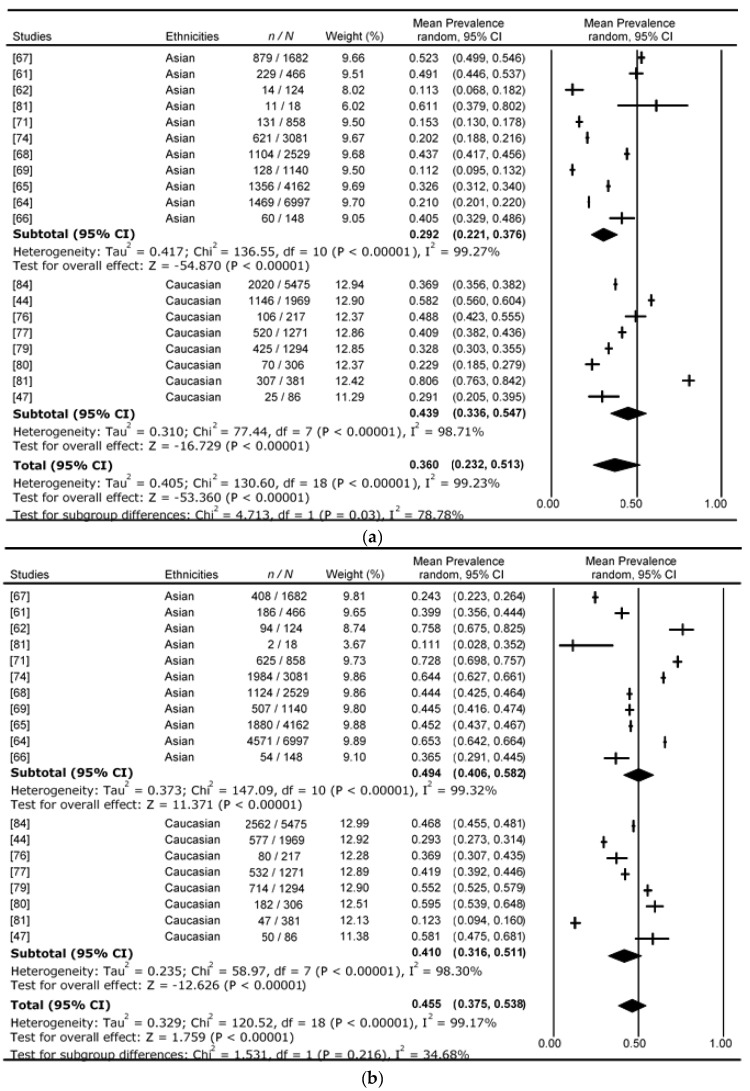
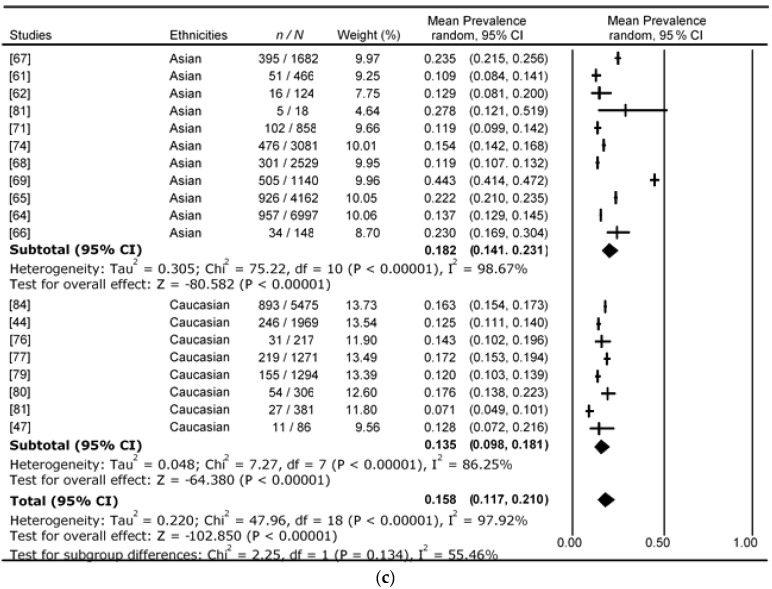
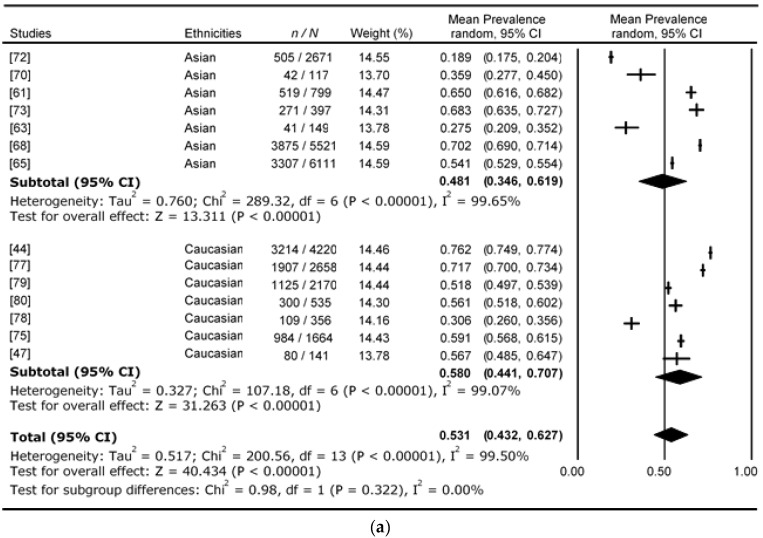
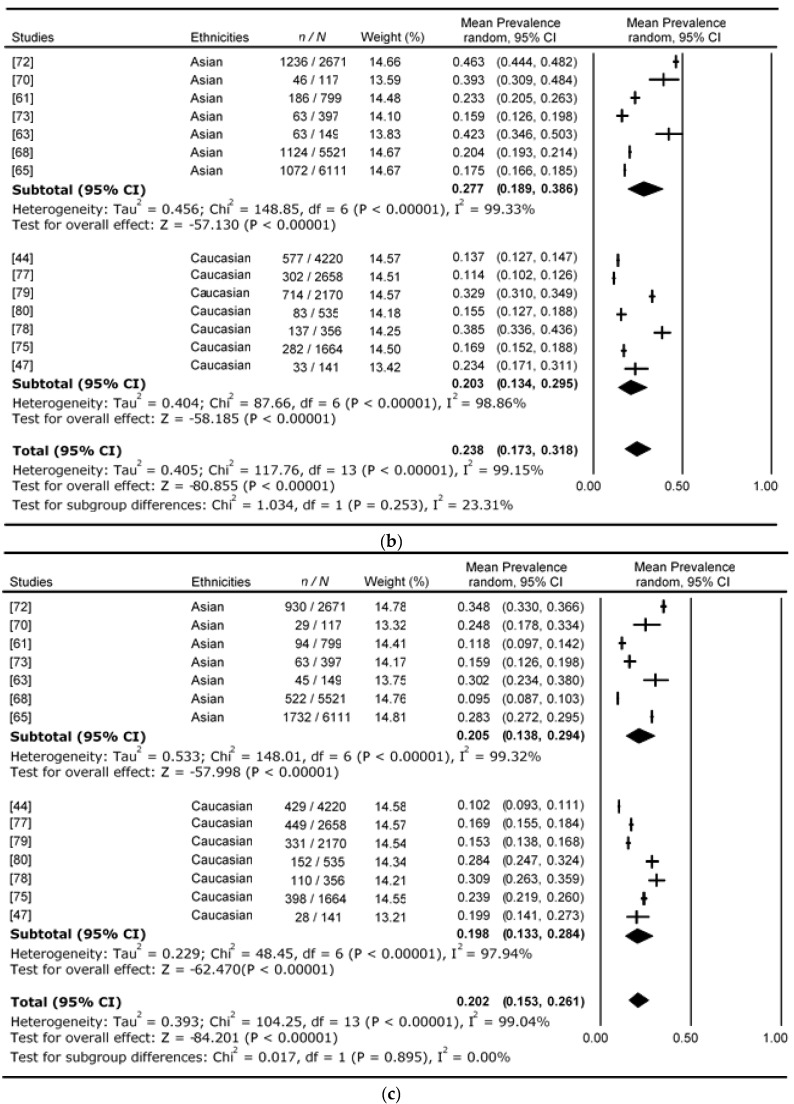
Prediabetes can be defined by the presence of impaired fasting glucose (IFG) and/or impaired glucose tolerance (IGT), or glycated haemoglobin (HbA1c) to identify individuals at increased risk of developing type 2 diabetes (T2D). The World Health Organization (WHO, 1999) and the American Diabetes Association (ADA, 2003) utilise different cut-off values for IFG (WHO: 6.1-6.9 mmol/L; ADA: 5.6-6.9 mmol/L) but the same cut-off values for IGT (7.8-11.0 mmol/L). This review investigates whether there are differences in prevalence of IFG, IGT, and combined IFG&IGT between ethnicities, in particular Asian Chinese and European Caucasians. In total, we identified 19 studies using the WHO1999 classification, for which the average proportional prevalence for isolated (i)-IFG, i-IGT, and combined IFG&IGT were 43.9%, 41.0%, and 13.5%, respectively, for Caucasian and 29.2%, 49.4%, and 18.2%, respectively, for Asian. For the 14 studies using ADA2003 classification, the average proportional i-IFG, i-IGT, and combined IFG&IGT prevalences were 58.0%, 20.3%, and 19.8%, respectively, for Caucasian; 48.1%, 27.7%, and 20.5%, respectively, for Asian. Whilst not statistically different, there may be clinically relevant differences in the two populations, with our observations for both classifications indicating that prevalence of i-IFG is higher in Caucasian cohorts whilst i-IGT and combined IFG&IGT are both higher in Asian cohorts.
Keywords: ethnicity; fasting plasma glucose; impaired fasting glucose; impaired glucose tolerance; obesity; oral glucose tolerance test; prediabetes; type 2 diabetes.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Lozano R., Naghavi M., Foreman K., Lim S., Shibuya K., Aboyans V., Abraham J., Adair T., Aggarwal R., Ahn S.Y., et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2095–2128. doi: 10.1016/S0140-6736(12)61728-0. - DOI - PMC - PubMed
-
- Danaei G., Finucane M.M., Lu Y., Singh G.M., Cowan M.J., Paciorek C.J., Lin J.K., Farzadfar F., Khang Y.H., Stevens G.A., et al. National, regional, and global trends in fasting plasma glucose and diabetes prevalence since 1980: Systematic analysis of health examination surveys and epidemiological studies with 370 country-years and 2.7 million participants. Lancet. 2011;378:31–40. doi: 10.1016/S0140-6736(11)60679-X. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
