

Prognostic Value of Clinical vs Pathologic Stage in Rectal Cancer Patients Receiving Neoadjuvant Therapy
- PMID: 29165692
- PMCID: PMC6279292
- DOI: 10.1093/jnci/djx228
Prognostic Value of Clinical vs Pathologic Stage in Rectal Cancer Patients Receiving Neoadjuvant Therapy
Abstract
Background: Neoadjuvant chemoradiation is currently standard of care in stage II-III rectal cancer, resulting in tumor downstaging for patients with treatment-responsive disease. However, the prognosis of the downstaged patient remains controversial. This work critically analyzes the relative contribution of pre- and post-therapy staging to the anticipated survival of downstaged patients.
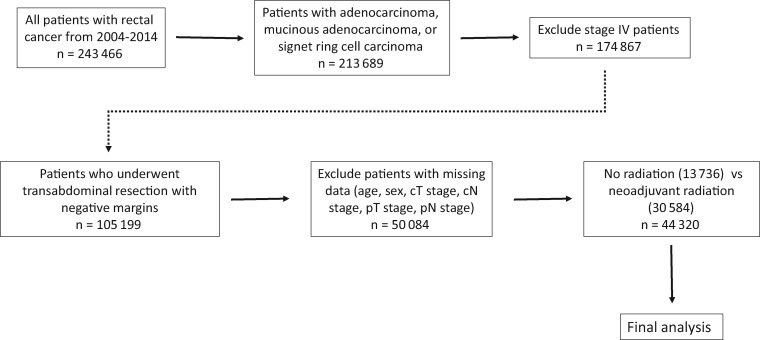
Methods: The National Cancer Database (NCDB) was queried for patients with rectal cancer treated with transabdominal resection between 2004 and 2014. Stage II-III patients downstaged with neoadjuvant radiation were compared with stage I patients treated with definitive resection alone. Patients with positive surgical margins were excluded. Overall survival was evaluated using both Kaplan-Meier analyses and Cox proportional hazards models. All statistical tests were two-sided.
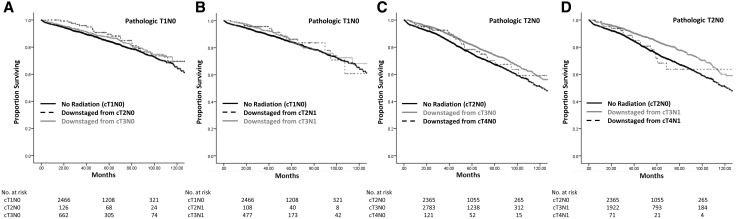
Results: A total of 44 320 patients were eligible for analysis. Survival was equivalent for patients presenting with cT1N0 disease undergoing resection (mean survival = 113.0 months, 95% confidence interval [CI] = 110.8 to 115.3 months) compared with those downstaged to pT1N0 from both cT3N0 (mean survival = 114.9 months, 95% CI = 110.4 to 119.3 months, P = .12) and cT3N1 disease (mean survival = 115.4 months, 95% CI = 110.1 to 120.7 months, P = .22). Survival statistically significantly improved in patients downstaged to pT2N0 from cT3N0 disease (mean survival = 109.0 months, 95% CI = 106.7 to 111.2 months, P < .001) and cT3N1 (mean survival = 112.8 months, 95% CI = 110.0 to 115.7 months, P < .001), compared with cT2N0 patients undergoing resection alone (mean survival = 100.0 months, 95% CI = 97.5 to 102.5 months). Multiple survival analysis confirmed that final pathologic stage dictated long-term outcomes in patients undergoing neoadjuvant radiation (hazard ratio [HR] of pT2 = 1.24, 95% CI = 1.10 to 1.41; HR of pT3 = 1.81, 95% CI = 1.61 to 2.05; HR of pT4 = 2.72, 95% CI = 2.28 to 3.25, all P ≤ .001 vs pT1; HR of pN1 = 1.50, 95% CI = 1.41 to 1.59; HR of pN2 = 2.17, 95% CI = 2.00 to 2.35, both P < .001 vs pN0); while clinical stage at presentation had little to no predictive value (HR of cT2 = 0.81, 95% CI = 0.69 to 0.95, P = .008; HR of cT3 = 0.83, 95% CI = 0.72 to 0.96, P = .009; HR of cT4 = 1.02, 95% CI = 0.85 to 1.21, P = .87 vs cT1; HR of cN1 = 0.96, 95% CI = 0.91 to 1.02, P = .19; HR of cN2 = 0.96, 95% CI = 0.86 to 1.08, P = .48 vs cN0).
Conclusions: Survival in patients with rectal cancer undergoing neoadjuvant radiation is driven by post-therapy pathologic stage, regardless of pretherapy clinical stage. These data will further inform prognostic discussions with patients.
Figures
References
-
- Siegel RL, Miller KD, Fedewa SA et al. , Colorectal cancer statistics, 2017. CA Cancer J Clin. 2017;67(3):177–193. - PubMed
-
- Rahib L, Smith BD, Aizenberg R et al. , Projecting cancer incidence and deaths to 2030: The unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014;74(11):2913–2921. - PubMed
-
- Minsky BD, Mies C, Recht A et al. , Resectable adenocarcinoma of the rectosigmoid and rectum. I. Patterns of failure and survival. Cancer. 1988;61(7):1408–1416. - PubMed
-
- Bosset JF, Collette L, Calais G et al. , Chemotherapy with preoperative radiotherapy in rectal cancer. N Engl J Med. 2006;355(11):1114–1123. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
