

Highly Accurate Identification of Cystic Precursor Lesions of Pancreatic Cancer Through Targeted Mass Spectrometry: A Phase IIc Diagnostic Study
- PMID: 29166170
- PMCID: PMC5805478
- DOI: 10.1200/JCO.2017.73.7288
Highly Accurate Identification of Cystic Precursor Lesions of Pancreatic Cancer Through Targeted Mass Spectrometry: A Phase IIc Diagnostic Study
Abstract
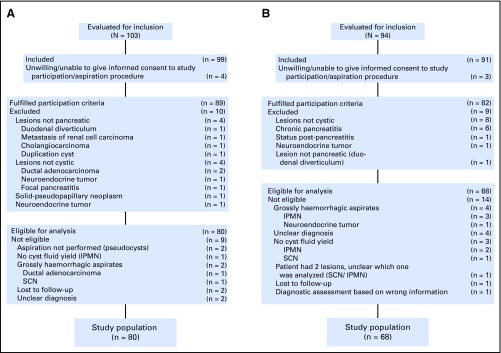
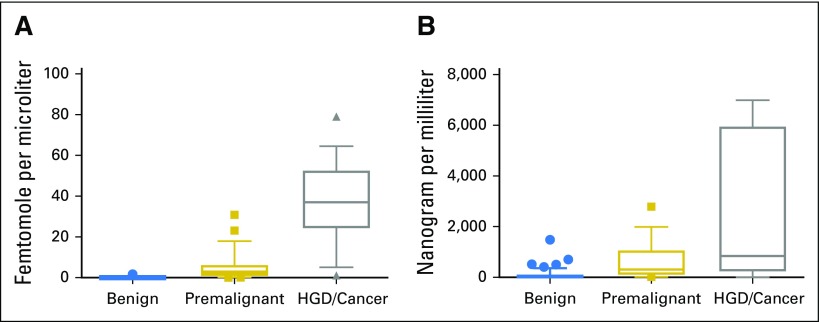
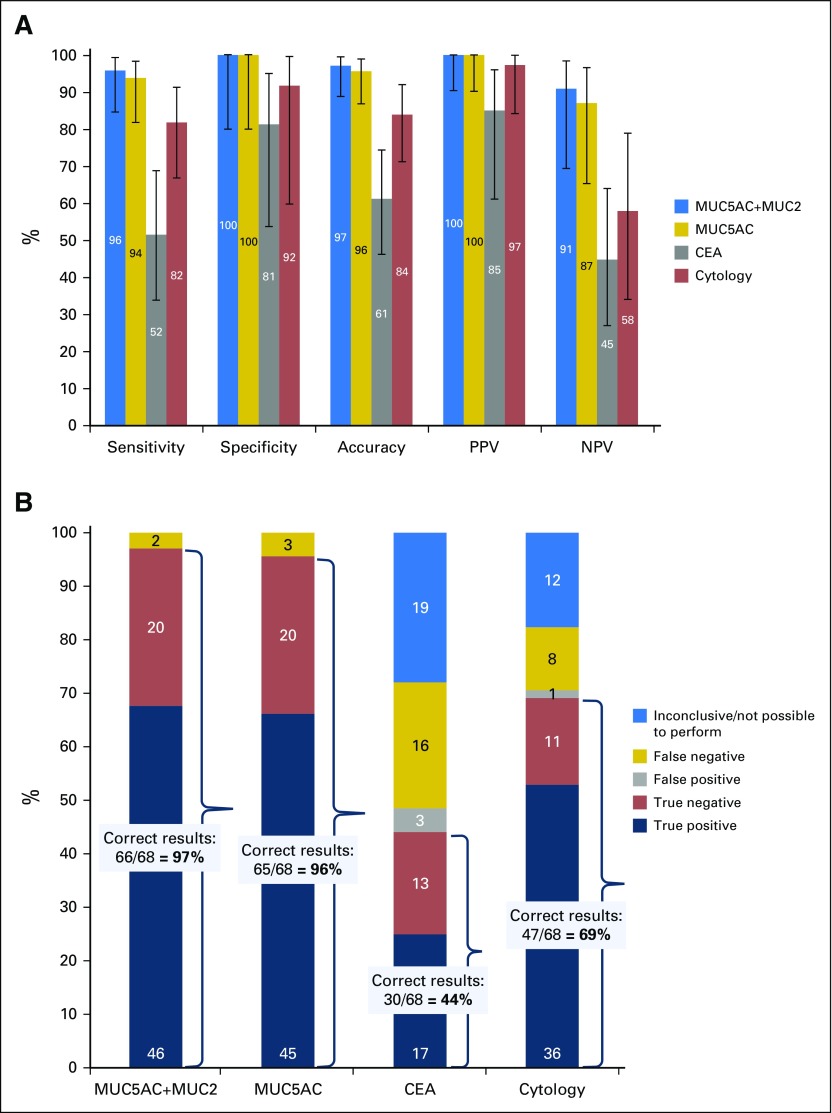
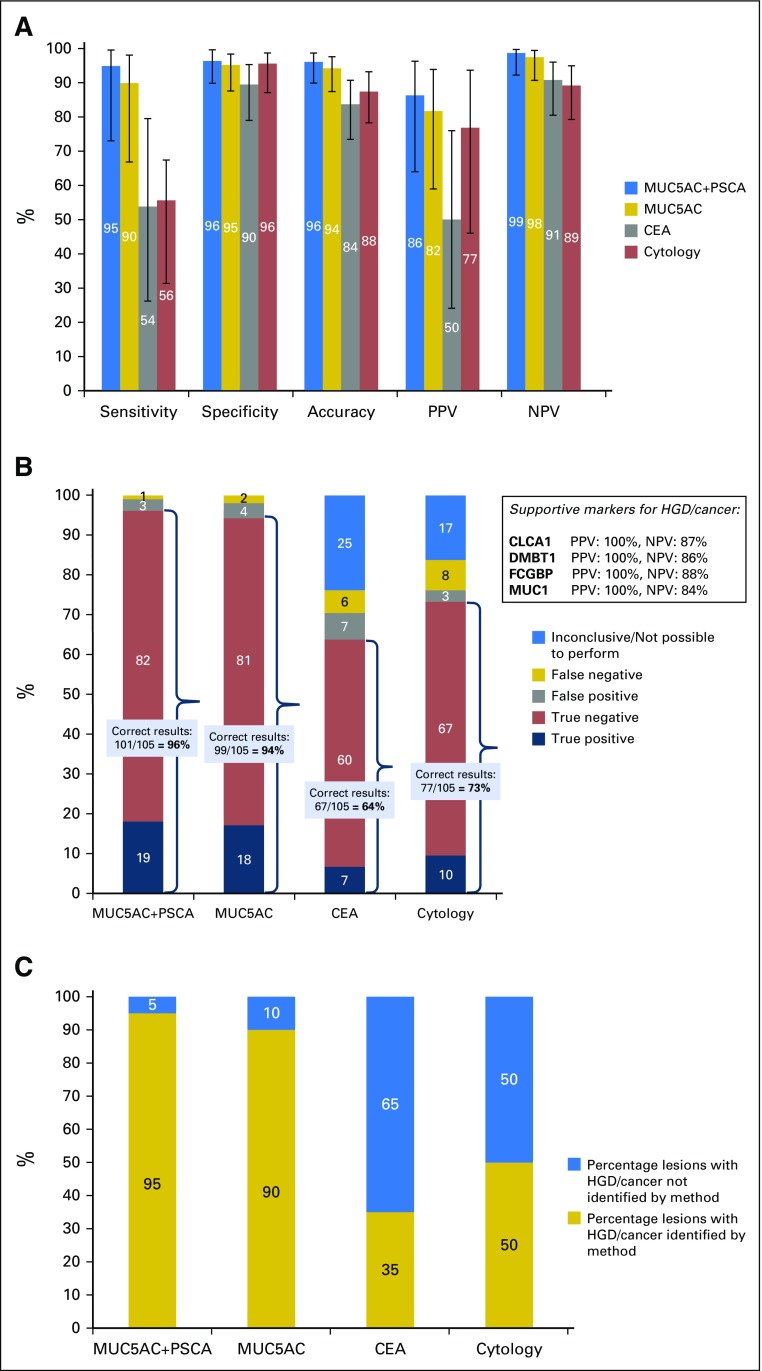
Purpose Pancreatic cystic lesions are common incidental findings on imaging, but up to half may be forerunners of pancreatic cancer. Therefore, accurate differential diagnosis is crucial for correct patient management. Unfortunately, currently available diagnostic methods cannot robustly identify premalignant and malignant pancreatic cystic lesions. Methods Cyst fluid samples obtained by routine endoscopic ultrasound-guided aspiration were used for the analyses. In a cohort of 24 patients, eight biomarker candidates for malignant potential and high-grade dysplasia/cancer were identified by an explorative proteomic approach. Subsequently, a quantitative analysis, using 30 heavy-labeled peptides from the biomarkers and parallel reaction monitoring mass spectrometry, was devised, tested in a training cohort of 80, and prospectively evaluated in a validation cohort of 68 patients. End points were surgical pathology diagnosis/clinical follow-up. Diagnostic assessments were blinded to mass spectrometry results. Results The optimal set of markers for detecting malignant potential was a panel of peptides from mucin-5AC and mucin-2, which could discriminate premalignant/malignant lesions from benign with an accuracy of 97% (95% CI, 89% to 99%) in the validation cohort. This result compared favorably with the accuracy of standard analyses: cyst fluid carcinoembryonic antigen (61%; 95% CI, 46% to 74%; P < .001) and cytology (84%; 95% CI, 71% to 92%; P = .02). A combination of proteins mucin-5AC and prostate stem-cell antigen could identify high-grade dysplasia/cancer with an accuracy of 96% (95% CI, 90% to 99%), and detected 95% of malignant/severely dysplastic lesions, compared with 35% and 50% for carcinoembryonic antigen and cytology ( P < .001 and P = .003, respectively). Conclusion Targeted mass spectrometry analysis of just three cyst fluid biomarkers provides highly accurate identification and assessment of cystic precursors to pancreatic adenocarcinoma. Additional studies should determine whether the method can facilitate timely cancer diagnosis, successful intervention, and prevention.
Figures
Comment in
-
Pancreatic cancer: Mass spectrometry indicates malignant potential.Nat Rev Clin Oncol. 2018 Feb;15(2):67. doi: 10.1038/nrclinonc.2017.199. Epub 2017 Dec 12. Nat Rev Clin Oncol. 2018. PMID: 29231193 No abstract available.
Similar articles
-
Proteomic mucin profiling for the identification of cystic precursors of pancreatic cancer.J Natl Cancer Inst. 2014 Feb;106(2):djt439. doi: 10.1093/jnci/djt439. J Natl Cancer Inst. 2014. PMID: 24523528 Free PMC article.
-
Accuracy of endoscopic ultrasound-guided fine needle aspiration cytology on the differentiation of malignant and benign pancreatic cystic lesions: a single-center experience.J Dig Dis. 2013 Mar;14(3):132-9. doi: 10.1111/1751-2980.12014. J Dig Dis. 2013. PMID: 23167591
-
Simple mucinous cyst: another potential cancer precursor in the pancreas? Case report with molecular characterization and systematic review of the literature.Virchows Arch. 2021 Jul;479(1):179-189. doi: 10.1007/s00428-021-03029-1. Epub 2021 Jan 28. Virchows Arch. 2021. PMID: 33511431 Free PMC article.
-
Cyst fluid carcinoembryonic antigen is an accurate diagnostic marker of pancreatic mucinous cysts.Pancreas. 2011 Oct;40(7):1024-8. doi: 10.1097/MPA.0b013e31821bd62f. Pancreas. 2011. PMID: 21775920
-
KRAS in Cyst Fluid Obtained by Endoscopic Ultrasound-Fine-Needle Aspiration in Pancreatic Cystic Lesions: A Systematic Review and Meta-analysis.Pancreas. 2019 Jul;48(6):749-758. doi: 10.1097/MPA.0000000000001325. Pancreas. 2019. PMID: 31206466
Cited by
-
Diagnosis and management of pancreatic cystic neoplasms.Frontline Gastroenterol. 2019 Jul;10(3):300-308. doi: 10.1136/flgastro-2018-101122. Epub 2019 Mar 1. Frontline Gastroenterol. 2019. PMID: 31288258 Free PMC article. Review.
-
Signal-Targeted Therapies and Resistance Mechanisms in Pancreatic Cancer: Future Developments Reside in Proteomics.Cancers (Basel). 2018 Jun 1;10(6):174. doi: 10.3390/cancers10060174. Cancers (Basel). 2018. PMID: 29865155 Free PMC article. Review.
-
Proteomic biomarkers in body fluids associated with pancreatic cancer.Oncotarget. 2018 Mar 27;9(23):16573-16587. doi: 10.18632/oncotarget.24654. eCollection 2018 Mar 27. Oncotarget. 2018. PMID: 29662668 Free PMC article. Review.
-
Early neoplastic lesions of the pancreas: initiation, progression, and opportunities for precancer interception.J Clin Invest. 2025 Jul 15;135(14):e191937. doi: 10.1172/JCI191937. eCollection 2025 Jul 15. J Clin Invest. 2025. PMID: 40662372 Free PMC article. Review.
-
Advances on diagnostic biomarkers of pancreatic ductal adenocarcinoma: A systems biology perspective.Comput Struct Biotechnol J. 2020 Nov 21;18:3606-3614. doi: 10.1016/j.csbj.2020.11.018. eCollection 2020. Comput Struct Biotechnol J. 2020. PMID: 33304458 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
