

Maternal complications and cesarean section without indication: systematic review and meta-analysis
- PMID: 29166440
- PMCID: PMC5697917
- DOI: 10.11606/S1518-8787.2017051000389
Maternal complications and cesarean section without indication: systematic review and meta-analysis
Abstract
Objective: The objective of this study was to determine the risks of severe acute maternal complications associated with cesarean section without medical indication.
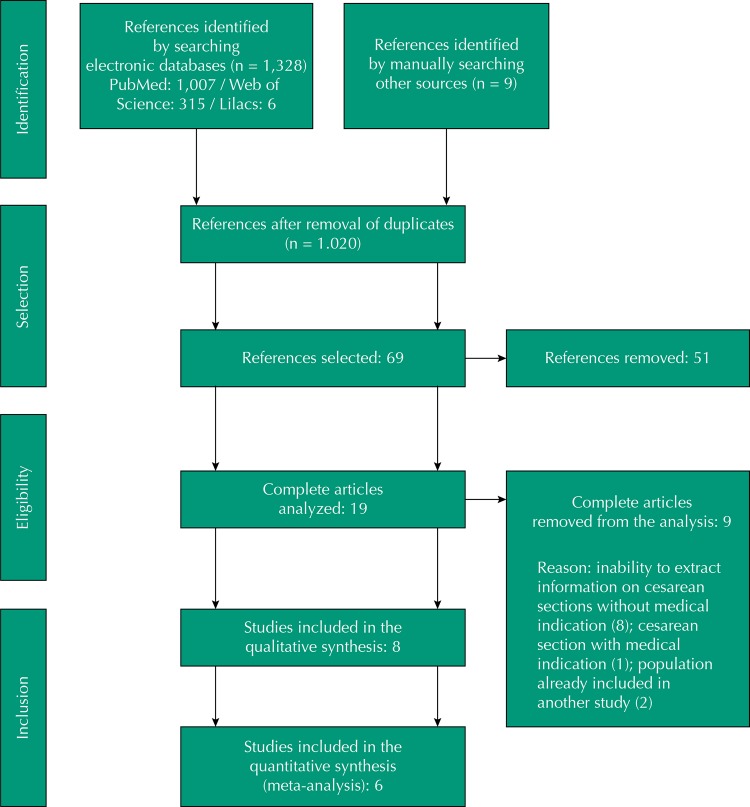
Methods: A systematic review was carried out with meta-analysis. The literature search was performed systematically, in multiple stages, in the PubMed, Lilacs, and Web of Science databases using the following descriptors: (postpartum period) and (cesarean section or natural childbirth) and ((morbidity or mortality) or (postpartum hemorrhage) or (puerperal infection) or (surgical infection) or (puerperal disorders)). The protocol of the study was registered at PROSPERO as CRD42016032933. A total of 1,328 articles were found; after selection, eight publications that met the study objective and inclusion criteria were selected, with information on 1,051,543 individuals.
Results: The results obtained in the meta-analyses indicate that women with cesarean section have a higher chance of maternal death (OR = 3.10, 95%CI 1.92-5.00) and postpartum infection (OR = 2.83, 95%CI, 1.585.06), but they have a lower chance of hemorrhage (OR = 0.52, 95%CI 0.48-0.57). For the blood transfusion outcome, the group effect was not associated with the type of delivery (95%CI 0.88-2.81).
Conclusions: The quality of evidence was considered low for hemorrhage and blood transfusion and moderate for postpartum infection and maternal death. Thus, cesarean sections should be performed with caution and safety, especially when its benefits outweigh the risks of a surgical procedure.
OBJETIVO: Determinar os riscos de complicações maternas agudas graves associadas ao parto cesárea sem indicação médica.
MÉTODOS: Foi conduzida uma revisão sistemática com meta-análise. A busca na literatura ocorreu de forma sistemática, em múltiplas etapas, nas bases de dados PubMed, Lilacs e Web of Science, utilizando os descritores: (postpartum period) and (cesarean section or natural childbirth) and ((morbidity or mortality) or (postpartum hemorrhage) or (puerperal infection) or (surgical infection) or (puerperal disorders)). O protocolo de estudo foi registrado na PROSPERO sob o número CRD42016032933. Foram encontrados 1.328 artigos, permanecendo, após seleção, oito publicações que atendiam ao objetivo do estudo e critérios de inclusão, com informações de 1.051.543 indivíduos.
RESULTADOS: Os resultados obtidos nas meta-análises indicam que mulheres de parto cesárea tem maior chance de morte materna (OR = 3,10; IC95% 1,92–5,00) e infecção pós-parto (OR = 2,83; IC95% 1,58–5,06), mas possuem menor chance de hemorragia (OR = 0,52; IC95% 0,48–0,57). Para o desfecho transfusão de sangue, o efeito agrupado não foi associado à via de parto (IC95% 0,88–2,81).
CONCLUSÕES: A qualidade da evidência foi considerada baixa para os desfechos hemorragia e transfusão de sangue e moderada para infecção pós-parto e morte materna. Assim, as cesáreas devem ser realizadas com prudência e segurança, principalmente quando seus benefícios superam os riscos de um procedimento cirúrgico.
Conflict of interest statement
Figures
References
-
- Allen VM, O’Connell CM, Baskett TF. Maternal morbidity associated with cesarean section without labor compared with induction of labor at term. Obstet Gynecol. 2006;108(2):286–294. https://doi.org/10.1097/01.AOG.0000215988.23224.e4. - DOI - PubMed
-
- Allen VM, O’Connell CM, Liston RM, Baskett TF. Maternal morbidity associated with cesarean section without labor compared with spontaneous onset of labor at term. Obstet Gynecol. 2003;102(3):477–482. https://doi.org/10.1016/S0029-7844(03)00570-2. - DOI - PubMed
-
- Althabe F, Belizan JM, Villar J, Alexander S, Bergel E, Ramos S, et al. Mandatory second opinion to reduce rates of unnecessary caesarean sections in Latin America: a cluster randomised controlled trial. Lancet. 2004;363(9425):1934–1940. https://doi.org/10.1016/S0140-6736(04)16406-4. - DOI - PubMed
-
- Azam S, Khanam A, Tirlapur S, Khan K. Planned caesarean section or trial of vaginal delivery? A meta-analysis. Curr Opin Obstet Gynecol. 2014;26(6):461–468. https://doi.org/10.1097/GCO.0000000000000114. - DOI - PubMed
-
- Béhague DP, Victora CG, Barros FC. Consumer demand for caesarean sections in Brazil: informed decision making, patient choice, or social inequality? A population based birth cohort study linking ethnographic and epidemiological methods. BMJ. 2002;324(7343):942–945. https://doi.org/10.1136/bmj.324.7343.942. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
