

Sporotrichosis: an update on epidemiology, etiopathogenesis, laboratory and clinical therapeutics
- PMID: 29166494
- PMCID: PMC5674690
- DOI: 10.1590/abd1806-4841.2017279
Sporotrichosis: an update on epidemiology, etiopathogenesis, laboratory and clinical therapeutics
Abstract
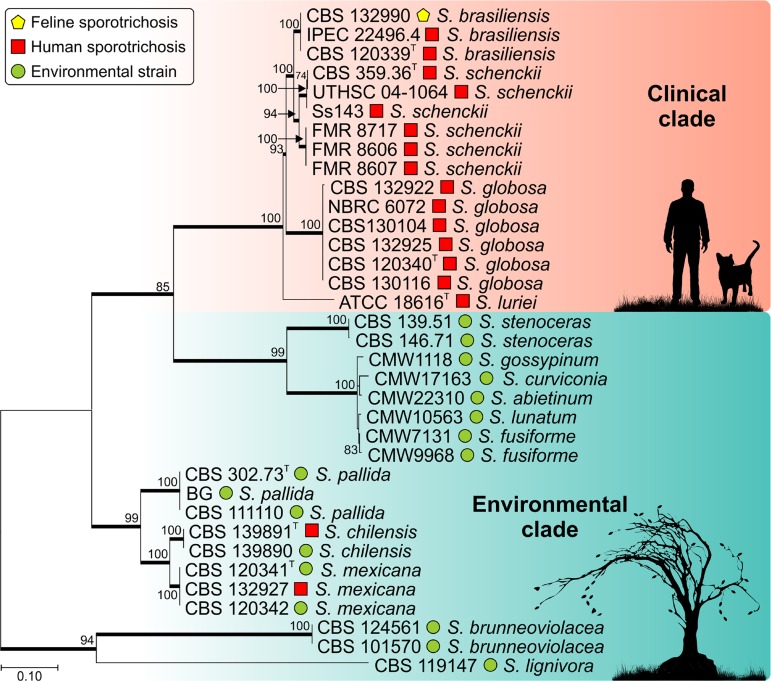
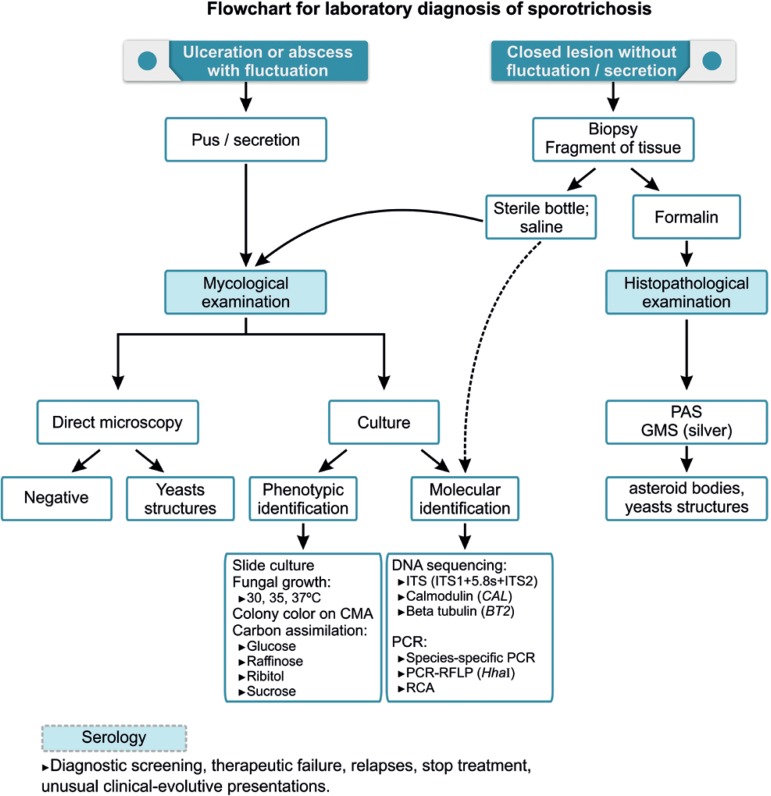
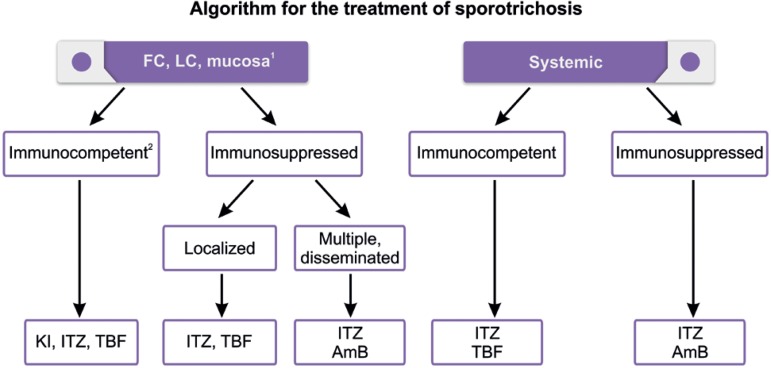
In the late 90's there was a change in both the route of transmission and the people at risk for sporotrichosis. This zoonotic cat-man alternative transmission route elicited changes in strategies to control the epidemic. There was a progressive increase in the number of cases involving especially children and the elderly. In addition to becoming hyperendemic, uncommon clinical pictures like immunoreactive clinical presentations or severe systemic cases have emerged. New species were identified and classified through molecular tools using more virulent clinical isolates, like S. brasiliensis, compared to the environmental isolates. Likewise, different species of Sporothrix have been associated with different geographic regions. The serological and molecular techniques are used as an auxiliary tool for the diagnosis and/or for species identification, although the isolation and the identification of Sporothrix spp. in clinical specimen is still the gold standard. Currently sporotrichosis epidemics requires the knowledge of the epidemiological-molecular profile to control the disease and the specific treatment. Itraconazole, potassium iodide, terfinafine, and amphotericin B are the available drugs in Brazil to treat sporotrichosis. The drug of choice, its posology, and treatment duration vary according to the clinical presentation, the Sporothrix species, and host immune status. New treatment choices, including a vaccine, are being developed; nevertheless, more clinical trials are required to confirm its efficacy.
Conflict of interest statement
Conflict of interests: None
Figures



References
-
- Conti Diaz IA. Epidemiology of sporotrichosis in Latin America. Mycopathologia. 1989;108:113–116. - PubMed
-
- Schenck BR. On refractory subcutaneous abscess caused by a fungus possibly related to the Sporotricha. Bull Johns Hopkins Hosp. 1898;93:286–290.
-
- Kwon-Chung KJ, Bennett JE. Sporotrichosis. In: Kwon-Chung KJ, Bennett JE, editors. Medical Mycology. Philadelphia: Lea & Febiger; 1992. pp. 707–729.
-
- Carmichael JW. Chrysosporium and some other aleuriosporic hyphomycetes. Can J Bot. 1962;40:1137–1173.
-
- Rodrigues AM, Kubitschek-Barreira PH, Fernandes GF, de Almeida SR, Lopes-Bezerra LM, de Camargo ZP. Immunoproteomic analysis reveals a convergent humoral response signature in the Sporothrix schenckii complex. J Proteomics. 2015 Feb 06;115:8–22. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous