

Anaphylaxis in an emergency care setting: a one year prospective study in children and adults
- PMID: 29166906
- PMCID: PMC5700668
- DOI: 10.1186/s13049-017-0402-0
Anaphylaxis in an emergency care setting: a one year prospective study in children and adults
Abstract
Background: Current data on anaphylaxis is based on retrospective and register based studies. The objective of this study was to describe the epidemiology of anaphylaxis in a 1 year prospective study at the emergency care setting, Odense University Hospital, Denmark (2013-2014).
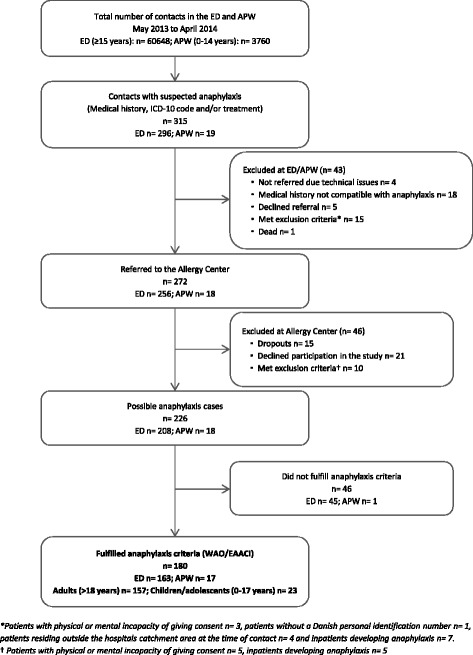
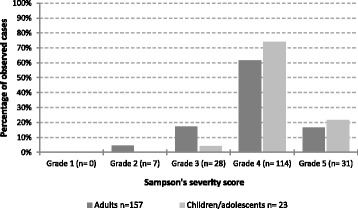
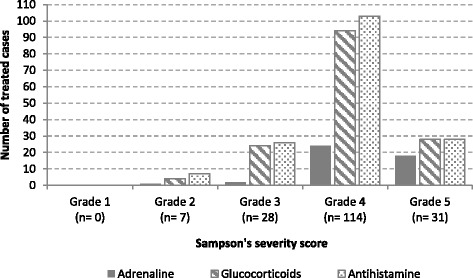
Methods: Prospective study at the emergency care setting, Odense University Hospital, Denmark (2013-2014). To identify anaphylaxis cases, records from all patients with clinical suspicion on anaphylaxis or a related diagnosis according to the International Classification of Diseases 10 and from patients treated at the emergency care setting or at prehospital level with adrenaline, antihistamines or glucocorticoids were reviewed daily. The identified cases were referred to the Allergy Center, where a standardized interview regarding the anaphylactic reaction was conducted. International guidelines were applied for the assessment of anaphylaxis and its pharmacological treatment. Severity of the anaphylactic reaction was evaluated according to Sampson's severity score.
Results: We identified 180 anaphylactic patients. Anaphylaxis represented 0.3%-0.4% of all contacts in the emergency care setting with an incidence rate of 26.8 cases per 100,000 person years (95% CI: 14.3-45.8) in children and 40.4 cases per 100,000 person years (95% CI: 32.8-49.3) in adults. Moderate to severe anaphylaxis was registered in 96% of the cases. Skin (96%) and respiratory (79%) symptoms were the most frequent registered, but 7% of cases in adults occurred without skin manifestations. The most common elicitor in children was food (61%), while drugs (48%) and venom (24%) were the main suspected elicitors in adults. Adrenaline was administered in 25% of the cases and it was significantly less administered than glucocorticoids (83%) and antihistamines (91%). The mortality rate during our study period was 0.3 cases per 100,000 person years.
Discussion: This is one of the first prospective studies on the epidemiology of anaphylaxis in children and adults, where the patients are identified not only based on diagnosis codes but also on history, symptoms and treatment and thereafter classified according to international diagnosis criteria for anaphylaxis. A limitation of this study is that only patients who gave consent to participate in the study were included. Furthermore, patients may have attended other hospitals during the study period. Therefore, the estimates are minimum figures.
Conclusion: The prospective study design with a broad search profile yield a higher incidence than previously reported. Adrenaline was administered in a low proportion of the patients with moderate to severe anaphylaxis. Standardized diagnosis criteria among physicians treating anaphylaxis are needed.
Keywords: Anaphylaxis; Epidemiology; Incidence; Prevalence; Symptoms; Treatment.
Figures
References
-
- Lieberman P, Camargo CA, Jr, Bohlke K, Jick H, Miller RL, Sheikh A, et al. Epidemiology of anaphylaxis: findings of the American college of allergy, asthma and immunology epidemiology of anaphylaxis working group. Ann Allergy Asthma Immunol. 2006;97(5):596–602. doi: 10.1016/S1081-1206(10)61086-1. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
