

Collaborative action for person-centred coordinated care (P3C): an approach to support the development of a comprehensive system-wide solution to fragmented care
- PMID: 29166917
- PMCID: PMC5700670
- DOI: 10.1186/s12961-017-0263-z
Collaborative action for person-centred coordinated care (P3C): an approach to support the development of a comprehensive system-wide solution to fragmented care
Abstract
Background: Fragmented care results in poor outcomes for individuals with complexity of need. Person-centred coordinated care (P3C) is perceived to be a potential solution, but an absence of accessible evidence and the lack of a scalable 'blue print' mean that services are 'experimenting' with new models of care with little guidance and support. This paper presents an approach to the implementation of P3C using collaborative action, providing examples of early developments across this programme of work, the core aim of which is to accelerate the spread and adoption of P3C in United Kingdom primary care settings.
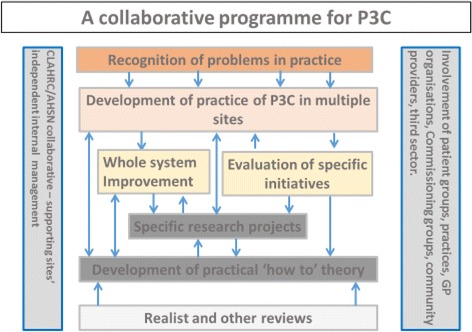
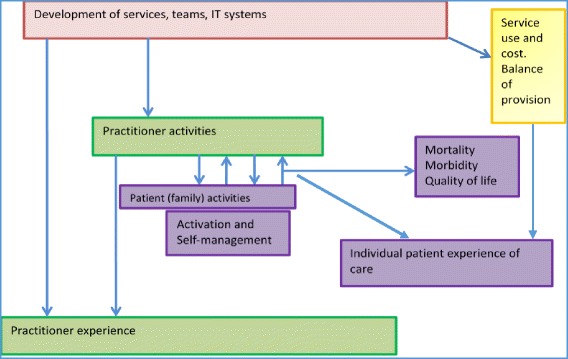
Methods: Two centrally funded United Kingdom organisations (South West Collaboration for Leadership in Applied Health Research and Care and South West Academic Health Science Network) are leading this initiative to narrow the gap between research and practice in this urgent area of improvement through a programme of service change, evaluation and research. Multi-stakeholder engagement and co-design are core to the approach. A whole system measurement framework combines outcomes of importance to patients, practitioners and health organisations. Iterative and multi-level feedback helps to shape service change while collecting practice-based data to generate implementation knowledge for the delivery of P3C. The role of the research team is proving vital to support informed change and challenge organisational practice. The bidirectional flow of knowledge and evidence relies on the transitional positioning of researchers and research organisations.
Results: Extensive engagement and embedded researchers have led to strong collaborations across the region. Practice is beginning to show signs of change and data flow and exchange is taking place. However, working in this way is not without its challenges; progress has been slow in the development of a linked data set to allow us to assess impact innovations from a cost perspective. Trust is vital, takes time to establish and is dependent on the exchange of services and interactions. If collaborative action can foster P3C it will require sustained commitment from both research and practice. This approach is a radical departure from how policy, research and practice traditionally work, but one that we argue is now necessary to deal with the most complex health and social problems.
Keywords: Collaborative action; Integration; Person-centred coordinated care.
Conflict of interest statement
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- Ryan J, Abrams MK, Doty MM, Shah T, Schneider EC. How high-need patients experience health care in the United States: findings from the 2016 Commonwealth Fund Survey of High-Need Patients. New York, NY: The Commonwealth Fund; 2016. - PubMed
-
- Curry N, Goodwin N, Naylor C, Robinson R. Practice based commissioning. Reinvigorate, replace or abandon? London: Kings Fund; 2008.
-
- Sheaff RHJ, Øvretveit J, Byng R, Exworthy M, Peckham S, et al. Integration and continuity of primary care: polyclinics and alternatives, an organisational analysis. Health Serv Deliv Res. 2015;3:35.
-
- National Voices. A Narrative for Person Centred Coordinated Care. 2013. https://www.nationalvoices.org.uk/publications/our-publications/narrativ....
-
- Royal College of Physicians . Putting the Pieces Together: Removing the Barriers to Excellent Patient Care. London: Royal College of Physicians; 2015.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
