

Large-scale proteomics identifies MMP-7 as a sentinel of epithelial injury and of biliary atresia
- PMID: 29167395
- PMCID: PMC5902315
- DOI: 10.1126/scitranslmed.aan8462
Large-scale proteomics identifies MMP-7 as a sentinel of epithelial injury and of biliary atresia
Abstract
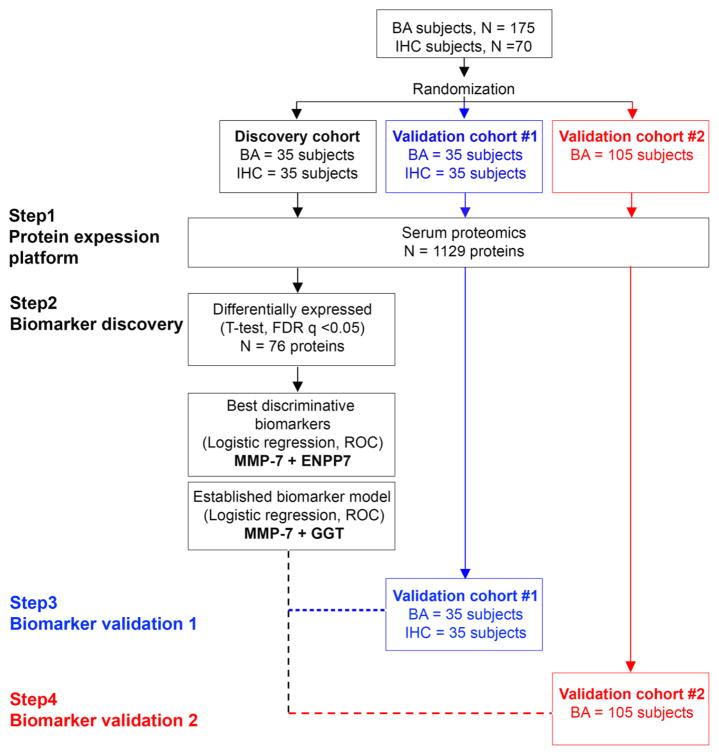
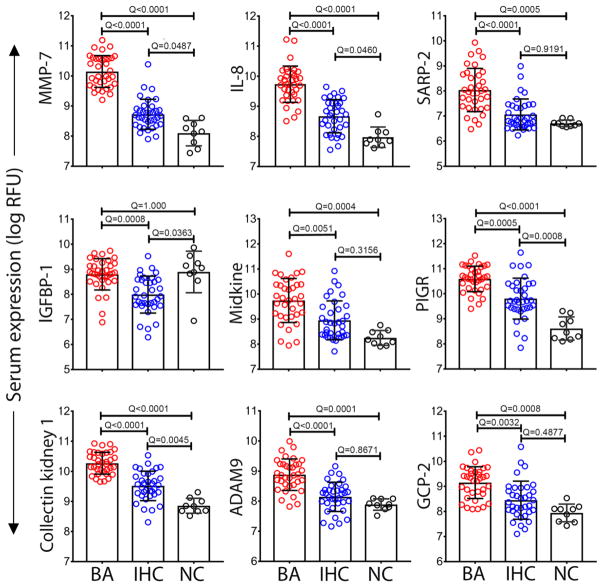
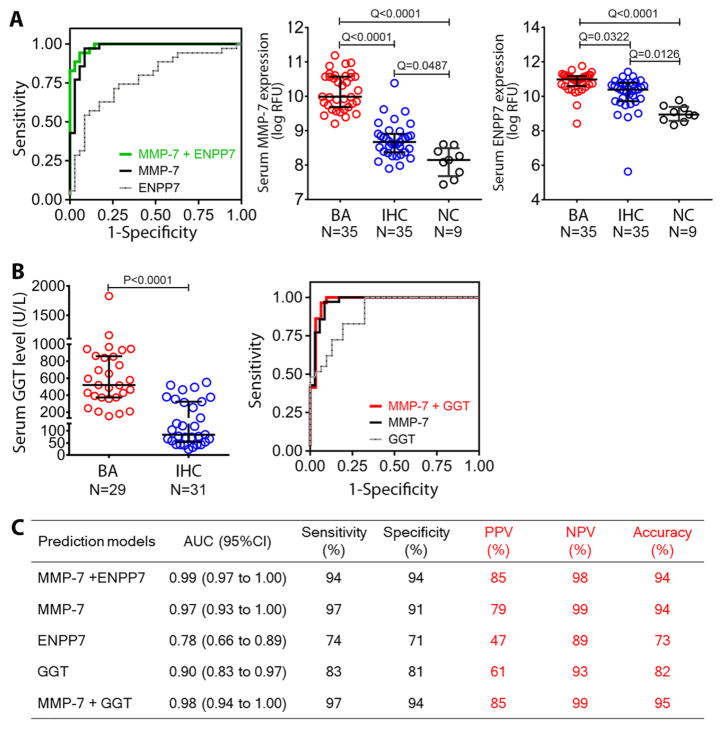
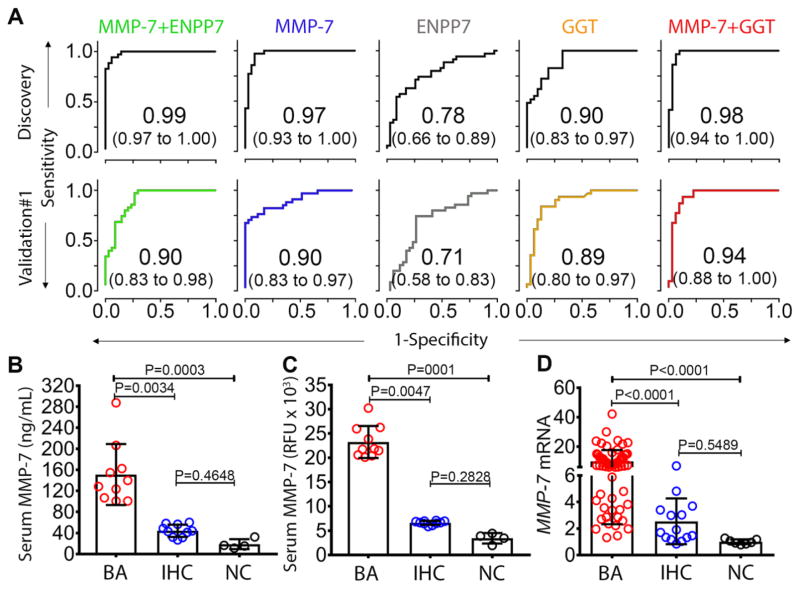
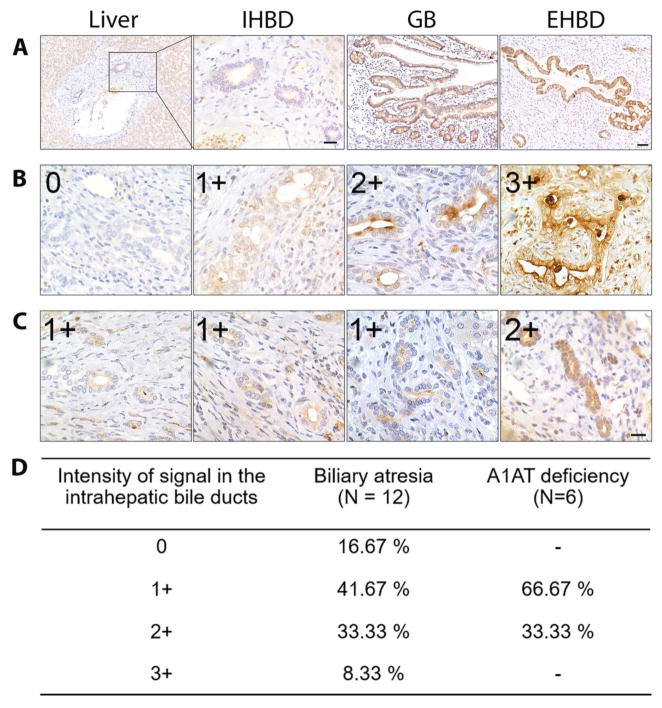
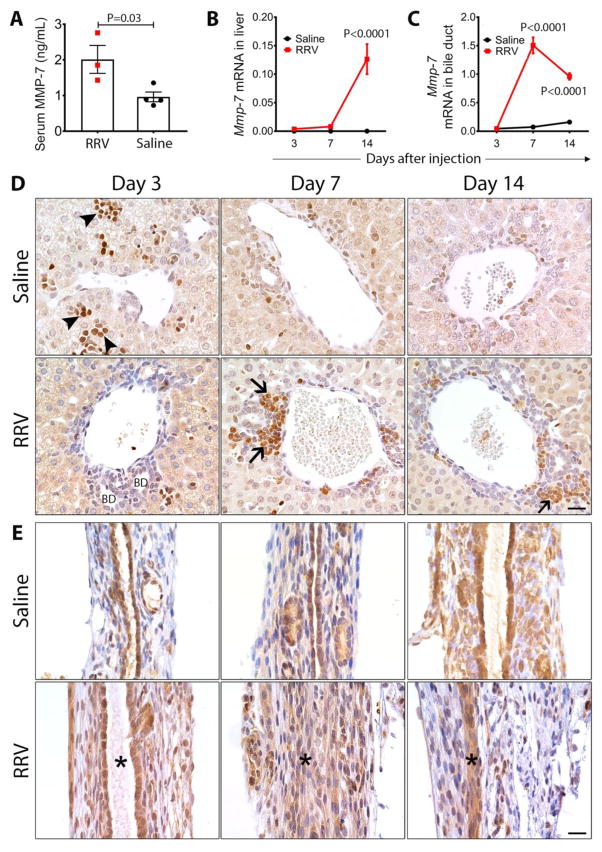
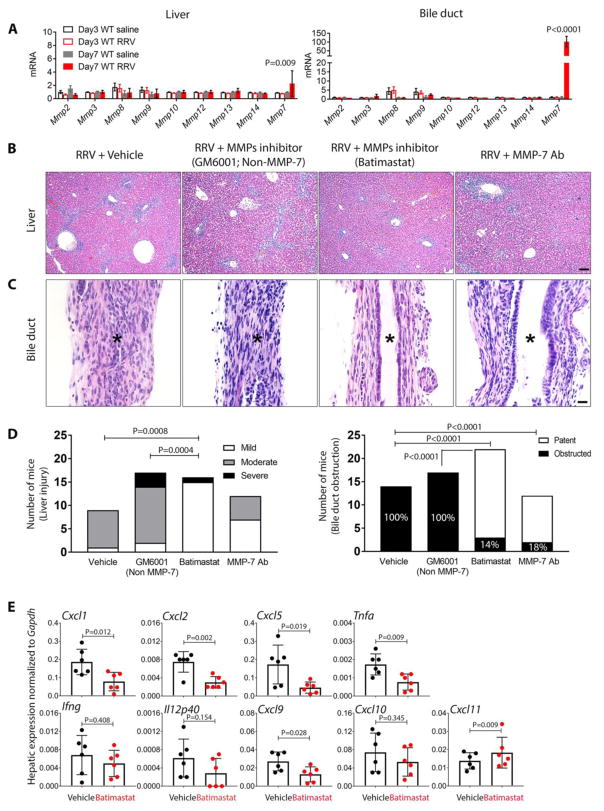
Biliary atresia is a progressive infantile cholangiopathy of complex pathogenesis. Although early diagnosis and surgery are the best predictors of treatment response, current diagnostic approaches are imprecise and time-consuming. We used large-scale, quantitative serum proteomics at the time of diagnosis of biliary atresia and other cholestatic syndromes (serving as disease controls) to identify biomarkers of disease. In a discovery cohort of 70 subjects, the lead biomarker was matrix metalloproteinase-7 (MMP-7), which retained high distinguishing features for biliary atresia in two validation cohorts. Notably, the diagnostic performance reached 95% when MMP-7 was combined with γ-glutamyltranspeptidase (GGT), a marker of cholestasis. Using human tissue and an experimental model of biliary atresia, we found that MMP-7 is primarily expressed by cholangiocytes, released upon epithelial injury, and promotes the experimental disease phenotype. Thus, we propose that serum MMP-7 (alone or in combination with GGT) is a diagnostic biomarker for biliary atresia and may serve as a therapeutic target.
Copyright © 2017 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works.
Conflict of interest statement
The authors declare no competing interests.
Figures
Comment in
-
Biliary tract: MMP7 - a diagnostic biomarker for biliary atresia.Nat Rev Gastroenterol Hepatol. 2018 Feb;15(2):68. doi: 10.1038/nrgastro.2017.175. Epub 2017 Dec 13. Nat Rev Gastroenterol Hepatol. 2018. PMID: 29235550 No abstract available.
References
-
- Yang Y, Muzny DM, Reid JG, Bainbridge MN, Willis A, Ward PA, Braxton A, Beuten J, Xia F, Niu Z, Hardison M, Person R, Bekheirnia MR, Leduc MS, Kirby A, Pham P, Scull J, Wang M, Ding Y, Plon SE, Lupski JR, Beaudet AL, Gibbs RA, Eng CM. Clinical whole-exome sequencing for the diagnosis of mendelian disorders. N Engl J Med. 2013;369:1502–1511. - PMC - PubMed
-
- Boyapati RK, Kalla R, Satsangi J, Ho GT. Biomarkers in Search of Precision Medicine in IBD. Am J Gastroenterol. 2016;111:1682–1690. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
